

Summary
Hospital readmissions are frequent (∼20% of patients admitted to the hospital are readmitted within 30 days of discharge) and expensive (∼$12 billion dollars/year). The Medicare Payment Advisory Committee has estimated that about 13.3% of these readmissions are preventable [Medicare Payment Advisory Commission. Medicare Payment Policy 2007]. The objective of the Hospital Readmissions Reduction Program is to reduce the rate of rehospitalization of Medicare patients for acute myocardial infarction, congestive heart failure, and pneumonia, and beginning in 2014, chronic obstructive pulmonary disease.
- Pneumonia
- Chronic Obstructive Pulmonary Disease
- Heart Failure
- Lower Respiratory Infections
- Myocardial Infarction
- Nursing
- Acute Lung Injury & Respiratory Failure
- Pneumonia
- Featured Meeting - Specialty page
- Chronic Obstructive Pulmonary Disease
- Heart Failure
- Exclusive Article - For home page
- Lower Respiratory Infections
- Pulmonary & Critical Care
- Myocardial Infarction
- Nursing
- Acute Lung Injury & Respiratory Failure
Hospital readmissions are frequent (∼20% of patients admitted to the hospital are readmitted within 30 days of discharge) and expensive (∼$12 billion dollars/year). The Medicare Payment Advisory Committee has estimated that about 13.3% of these readmissions are preventable [Medicare Payment Advisory Commission. Medicare Payment Policy 2007]. The objective of the Hospital Readmissions Reduction Program (HRRP) is to reduce the rate of rehospitalization of Medicare patients for acute myocardial infarction (AMI), congestive heart failure (CHF), and pneumonia, and beginning in 2014, chronic obstructive pulmonary disease (COPD).
There does not appear to be any specific intervention or bundle of interventions that will reliably reduce rehospitalization [Hansen LO et al. Ann Intern Med 2011]. David H. Au, MD, MS, University of Washington, Seattle, Washington, USA, said that reduction in rehospitalization must account for hospital and individual components, and the delivery and quality of outpatient care. Advanced care planning, continuity of follow-up, and access must also be considered (Table 1). He suggested that reducing hospital readmissions is an outcome of good health, so the most appropriate approach is to focus on improving health as a social issue as well as a hospital goal. To accomplish this we need to redesign and coordinate how the stakeholders interact [Kangovi S et al. JAMA 2011].
Conceptual Model
Jerry A. Krishnan, MD, PhD, University of Illinois Hospital and Health Sciences System, Chicago, Illinois, USA, discussed Project BOOST (Better Outcomes for Older Adults Through Safe Transitions) as an example of one initiative that is striving to improve the care of patients as they transition from hospital to home.
There are factors during the index hospitalization that can be addressed to reduce readmissions. Table 2 lists some of the concerns/evaluations that are addressed at each phase of the initial hospital stay as part of Project BOOST's General Assessment of Preparedness. The objective is to identify patients at risk for readmission, target interventions to avoid readmission, and improve the information flow between inpatient and outpatient providers.
Safe Transition Planning
A successful transition program requires careful planning and implementation and a process for ongoing monitoring and adjustment (Table 3). Development of the program should include the healthcare workers who interact with patients at all stages of their hospitalization and the staff of the facilities to which patients will transition. The development team should also include nutrition and dietary specialists, medical records technicians, and hospital data specialists and should consider the needs of the individuals who will be supporting the patient postdischarge. Dr. Krishnan suggested that input from former patients might also help to enhance the process.
Project Timeline
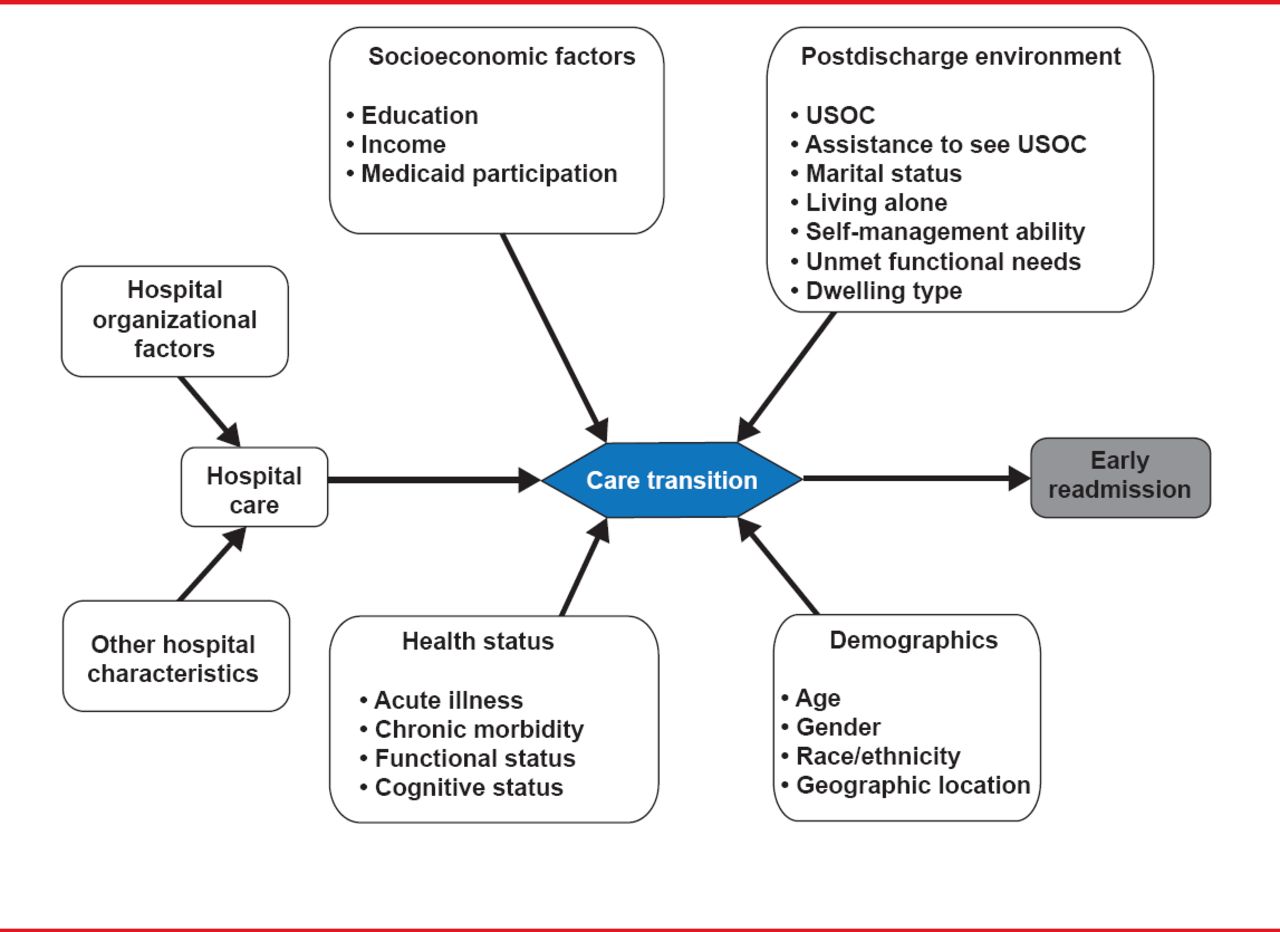
Although the HRRP assumes a relationship between adherence to the recommended hospital care processes and readmission rates, the results from several studies indicate a more complex problem. John Daryl Thornton, MD, MPH, Case Western Reserve University, Cleveland, Ohio, USA, examined predictors of readmission, specifically in respiratory patients. In one study, hospitals with greater adherence to recommended care processes did not achieve meaningfully better 30-day hospital readmission rates compared with those who had lower levels of performance [Stefan MS et al. J Gen Intern Med 2013]. Another study suggested minimizing preventable inpatient safety events and improving coordination of care between and across settings might decrease the likelihood of readmission [Rosen MK et al. Med Care 2013]. In a third study, length of stay (LoS; OR, 1.03; 95% CI, 1.01 to 1.05) and disease severity (OR, 1.67; 95% CI, 1.5 to 1.86) predicted readmission but not improved communication between inpatient and outpatient care teams (OR, 1.08; 95% CI, 0.92 to 1.26) [Oduyebo I et al. JAMA Intern Med 2013]. Finally, another recent study suggests that solely addressing the factors associated with the disease responsible for the index admission may not reduce readmissions. This is due to the fact that many of the patients were re-admitted for alternative diagnoses [Dharmarajan K et al. JAMA 2013]. Therefore, it is likely that multiple key components are working concomitantly to provoke readmissions including patient socioeconomic factors, demographics, and health status as well as the environment into which they are discharged (Figure 1) [Arbaje AI et al. Gerontologist 2008].

Factors That Influence Hospital Readmission
Source: Arbaje AI et al. Gerontologist 2008
Independent risk factors associated with an increased risk of rehospitalization for COPD include increasing age, male gender, any prior hospitalization, and comorbid asthma or pulmonary hypertension [McGhan R et al. Chest 2007]. There is also a relationship between malnutrition or weight loss during hospitalization and readmission for COPD [Zapatero A et al. J Hum Nutr Diet 2013; Pouw EM et al. Clin Nutr 2000]. A better understanding of the factors occurring outside of the hospital is needed to make a meaningful impact—a system level approach is key.
Medicare's switch to a diagnosis-related group system was a powerful incentive for hospitals to support strategies to reduce LoS and decrease hospital costs. It also contributed to the growth of “hospitalists”—specialists in inpatient medicine. Gulshan Sharma, MD, MPH, FCCP, University of Texas Medical Branch, Galveston, Texas, USA, discussed the hospitalist movement and its impact on the process of care and postdischarge outcomes.
In 2006, there were ∼10,000 hospitalists; in 2012 that number was ∼30,000. Results from a large retrospective study of >76,000 patients indicate that for common inpatient diagnoses (eg, pneumonia, congestive heart failure, chest pain, COPD), the hospitalist model is associated with a small reduction in LoS (0.4 days) and cost but no difference in in-hospital mortality or 14-day readmission rate [Lindenauer PK et al. N Engl J Med 2007]. More recently, hospitalist care was shown to be associated with decreased LoS (−0.64 days) and lower hospital costs (−$282) but higher 30-day post discharge cost (+$332; p<0.001 for both). These results were primarily associated with the fact that patients treated by hospitalists were less likely to be discharged to home (OR, 0.82; 95% CI, 0.78 to 0.86) and more likely to have emergency department visits (OR, 1.18; 95% CI, 1.12 to 1.24) and readmissions (OR, 1.08 95% CI, 1.02 to 1.14) [Kuo YF, Goodwin JS. Ann Intern Med 2011].
As for quality, one study indicated that the use of hospitalists was associated with modest improvement in process measures for acute myocardial infarction, CHF, or pneumonia [Vasilevskis EE et al. J Hosp Med 2010]. However, care by a hospitalist physician was not associated with better outcomes for these conditions [Goodrich K et al. J Hosp Med 2012]. It is likely that system level factors are more important than the hospitalist per se in improving quality and patient safety [Goodwin JS et al. J Gen Intern Med 2013].
David J Weidig, MD, Aurora Health Care, Milwaukee, Wisconsin, USA, discussed how key pre- and postdischarge planning initiatives successfully decrease hospital readmissions based on his experience as a hospitalist in a large healthcare system that used Project BOOST (Better Outcomes by Optimizing Safe Transitions).
Dr. Weidig reviewed the BOOST tools for addressing risk, including the “8P” risk stratification process (Table 4), the at-admission and pre-discharge General Assessment of Preparedness (GAP), and the BOOST Universal Discharge Checklist, which addresses the readiness of patients for transition out of the hospital. A final, but essential component is the 48-hour post-discharge call by physicians.
Boost 8Ps Assessment
Areas of potential integration and benefit include intensive care unit admission, and electronic medical records integration, patient satisfaction training for physicians, palliative care, skilled nursing facilities, visiting nurses, and the emergency department. A final, but essential component is the 48-hour postdischarge call by physicians.
Dr. Weidig noted, “It may take up to 18 months to start seeing results once an intervention is started. Interventions are interdependent so you may be doing well in one area and not see results because of weakness in another. Involvement from everyone on the healthcare delivery team is needed, BUT it must be a built-in part of the work day and culture.”

The editors would like to thank the many members of the American Thoracic Society presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.