

Summary
Renal denervation (RDN) is a novel treatment of resistant hypertension, based on the Renal Denervation in Patients with Uncontrolled Hypertension study [Symplicity HTN-2; Symplicity HTN-2 Investigators. Lancet 2010]. Yet, the magnitude and determinants of office and ambulatory blood pressure (BP) response to RDN have not been established. This article discusses the results of the first patient-level meta-analysis of the BP changes 6 months post RDN at 10 expert centers participating in the European Network Coordinating Research on Renal Denervation study [ENCOReD].
- Renal Disease
- Interventional Radiology
- Hypertension & Kidney Disease
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Hypertensive Disease
- Renal Disease
- Cardiology & Cardiovascular Medicine
- Interventional Radiology
- Hypertension & Kidney Disease
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Hypertensive Disease
Renal denervation (RDN) is a novel treatment of resistant hypertension, based on the Renal Denervation in Patients With Uncontrolled Hypertension study [Symplicity HTN-2; Symplicity HTN-2 Investigators. Lancet 2010]. Yet, the magnitude and determinants of office and ambulatory blood pressure (BP) response to RDN have not been established due to the lack of randomized studies, few reports of postprocedural changes in ambulatory BP (or their lack of significance), and publication bias [Persu A et al. Expert Rev Cardiovasc Ther 2013].
Alexandre Persu, MD, Université Catholique de Louvain, Brussels, Belgium, presented the results of the first patient-level meta-analysis of the BP changes 6 months post RDN at 10 expert centers participating in the European Network Coordinating Research on Renal Denervation study [ENCOReD].
The study objective was to compare the BP changes in the ENCOReD RDN patients and those observed in the treatment and placebo arms of the Systolic Hypertension in Europe study [Syst-Eur; Staessen JA et al. J Hypertens 1994; Staessen JA et al. Lancet 1997], and the Symplicity HTN-2 study.
For the comparison with Syst-Eur, the three patient groups were ENCOReD RDN (n=109), Syst-Eur placebo (n=73), and Syst-Eur active treatment (n=79). The RDN patients were younger than the other groups (mean age, 58.2 vs 71.4 vs 70.3 years, respectively), more overweight (body mass index, 29.5 vs 26.3 vs 26.0 kg/m2), and had more target organ damage. The estimated glomerular filtration rate was greater in the RDN group (RDN, 82.2 mL/min/1.73 m2; Syst-Eur placebo, 67.9 mL/min/1.73 m2; Syst-Eur active, 67.2 mL/min/1.73 m2). The baseline systolic BP (SBP) levels were similar for office (175 to 178 mm Hg) and ambulatory (153 to 157 mm Hg) measures. Nearly half of each group was women and nearly all were white.
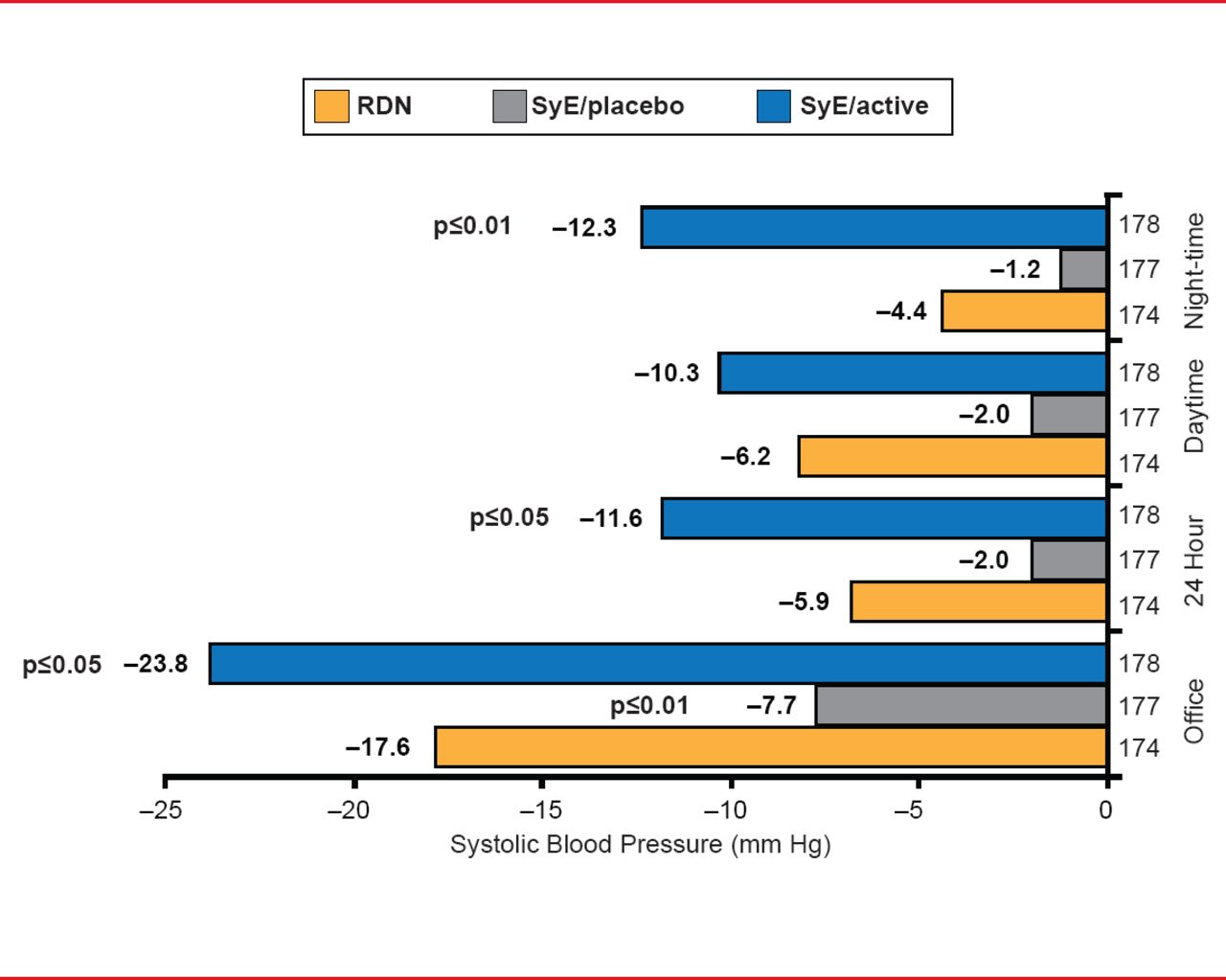
In the RDN group, the office SBP was reduced by 17.6 mm Hg and the 24-hour ambulatory SBP (ASBP) by 5.9 mm Hg from baseline to 6 months (p<0.03 for both) at 6 months. Reduction from baseline to 6 months in office, ambulatory, daytime, and night-time SBP values in the RDN group were between the respective values for the Syst-Eur placebo and Syst-Eur active groups (Figure 1). The reduction in ASBP was only one-third that on office BP measure. The less impressive decrease in ASBP may reflect a specific effect of RDN on white coat hypertension (WCH), noted Prof. Persu. WCH was decreased in each group.

Change From Baseline to 6 Months in SBP
RDN=renal denervation; SyE=Syst-Eur. p values for comparison with RDN group.
The nonresponder rate for a reduction in office SBP at 6 months was 23% for RDN, 33% for Syst-Eur placebo, and 8% for Syst-Eur active. The nonresponder rate for ASBP at 6 months was 35% in the RDN, 45% in the Syst-Eur placebo, and 17% in the Syst-Eur active group.
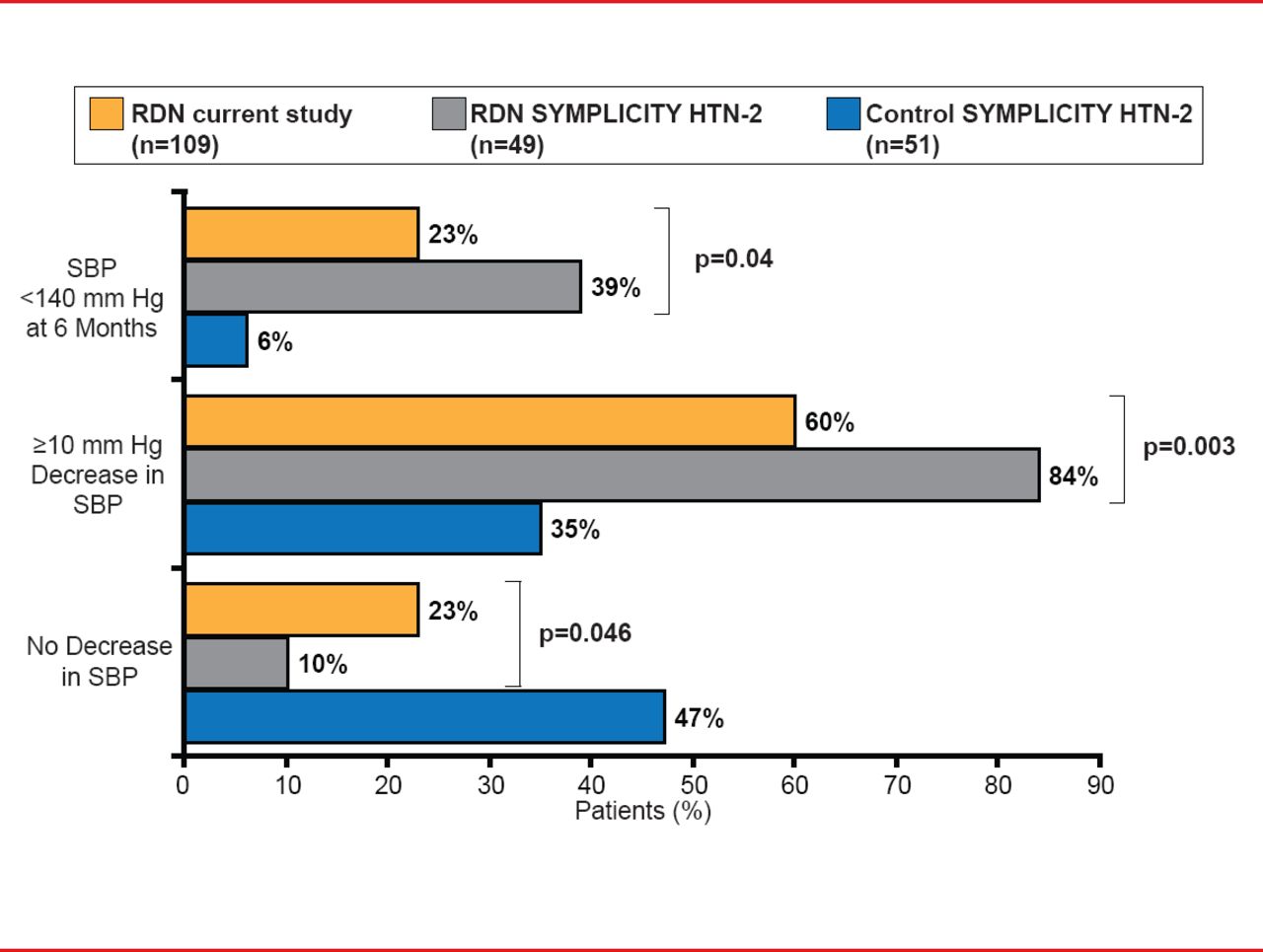
Compared with the RDN group in Symplicity HTN-2, there was a significantly lower proportion of responders and controlled patients in the ENCOReD RDN group at 6 months (p=0.003 and p=0.04, respectively; Figure 2). For the patients with a baseline SBP ≥160 mm Hg, the responder rate at 6 months was similar in the ENCOReD and Symplicity HTN-2 RDN groups (72% vs 84%; p=0.12), but significantly fewer ENCOReD RDN patients had BP control (16% vs 39%; p=0.005).

BP Response Over 6 Months in RDN and Symplicity HTN-2 Patients
RDN=renal denervation; SBP=systolic blood pressure.
In ENCOReD RDN patients, a higher baseline SBP predicted better 24-hour ASBP control, whereas a higher serum creatinine predicted a lower probability of control.
The meta-analysis suggests an important impact of the placebo or Hawthorne effects, and/or regression to the mean. RDN should be the last resort for truly resistant hypertension until there is sufficient evidence to identify reliable predictors of BP response.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.