

Summary
This article discusses results from a European study, demonstrating that although the management of patients with atrial fibrillation (AF) has changed based on updated guidelines, many continue to experience symptoms, highlighting the need to improve the management of this patient population. The Prevention of Thromboembolic Events - European Registry in Atrial Fibrillation [PREFER in AF] is a multicenter study conducted across seven countries in Europe, comprising a prospective, observational disease registry. The study was designed to determine the extent to which publication of the 2010 European Society of Cardiology guidelines has affected clinical behavior in Europe.
- Cardiology Clinical Trials
- Exclusive Article - For home page
- Arrhythmias
- Cardiology Guidelines
- Cardiology Clinical Trials
- Exclusive Article - For home page
- Arrhythmias
- Cardiology Guidelines
- Cardiology
Paulus Kirchhof, MD, University of Birmingham, Birmingham, United Kingdom, presented results from a European study, demonstrating that although the management of patients with atrial fibrillation (AF) has changed based on updated guidelines, many continue to experience symptoms, highlighting the need to improve the management of this patient population.
The Prevention of Thromboembolic Events - European Registry in Atrial Fibrillation [PREFER in AF] is a multicenter study conducted across seven countries in Europe, comprising a prospective, observational disease registry. The study was designed to determine the extent to which publication of the 2010 European Society of Cardiology (ESC) guidelines has affected clinical behavior in Europe.
Inclusion criteria were patient age of at least 18 years; a history of AF documented by some form of recording of electrical activity of the heart within the previous 12 months; and written, informed consent to participate in the study. The registry enrolled 7243 patients (60% men; mean age 71.5 years; 72% with hypertension; 23% with coronary artery disease; 8% with prior stroke; 11% with prior myocardial infarction; and 4% with valvular AF). Patients were evaluated at an initial baseline visit to investigate their symptoms and disease-management strategies, with an emphasis on preventing thromboembolic events. A follow-up visit will occur 12 months after the baseline visit.
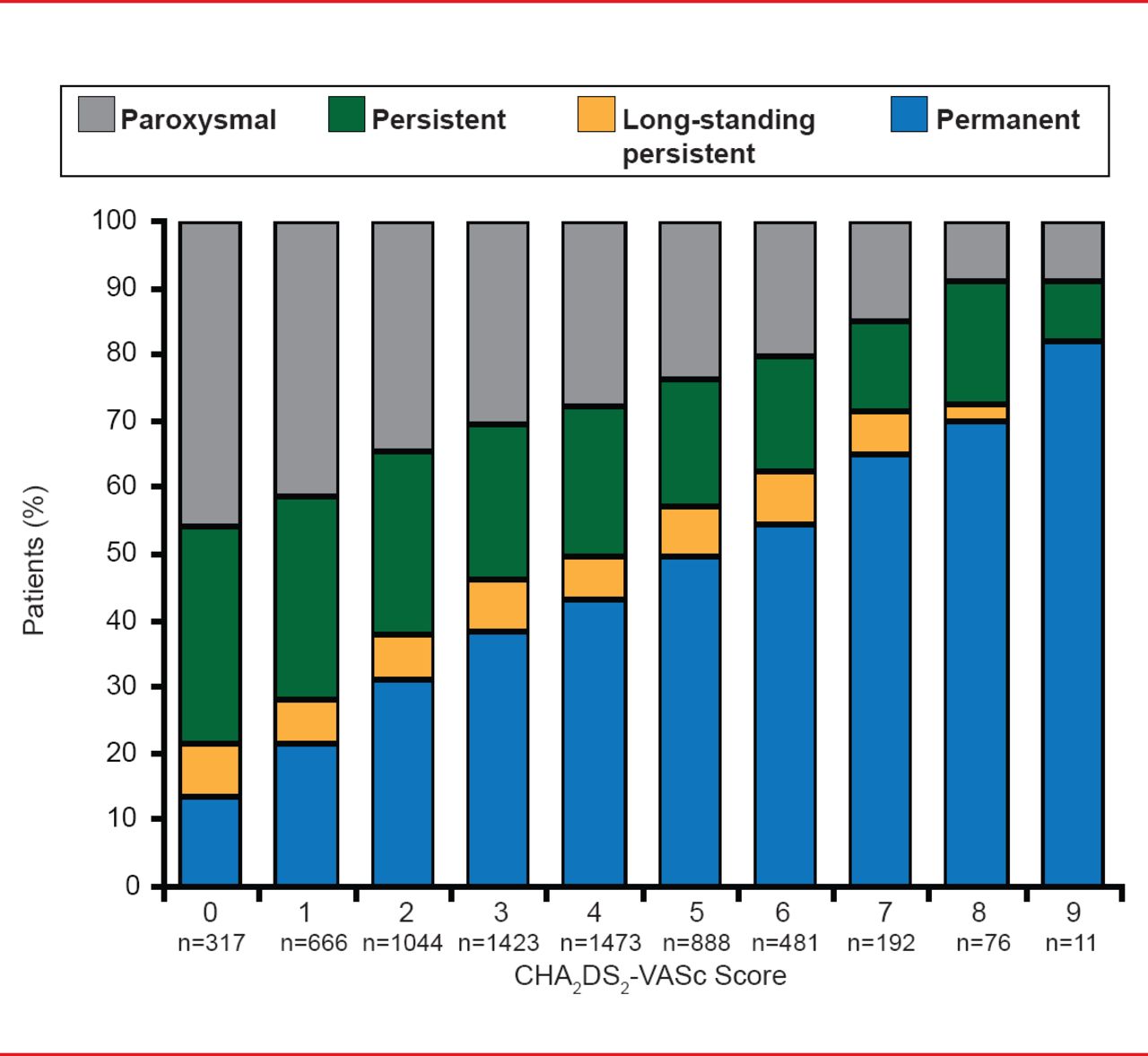
At baseline it was demonstrated that as CHA2DS2-VASc scores increase, so does the incidence of chronic forms of AF (persistent, long-standing persistent, and permanent). Conversely, the proportion of paroxysmal AF patients is reduced as scores increase (Figure 1).

Relationship Between Type of AF and CHA2DS2-VASc Score
Reproduced with permission from P Kirchhof, MD.
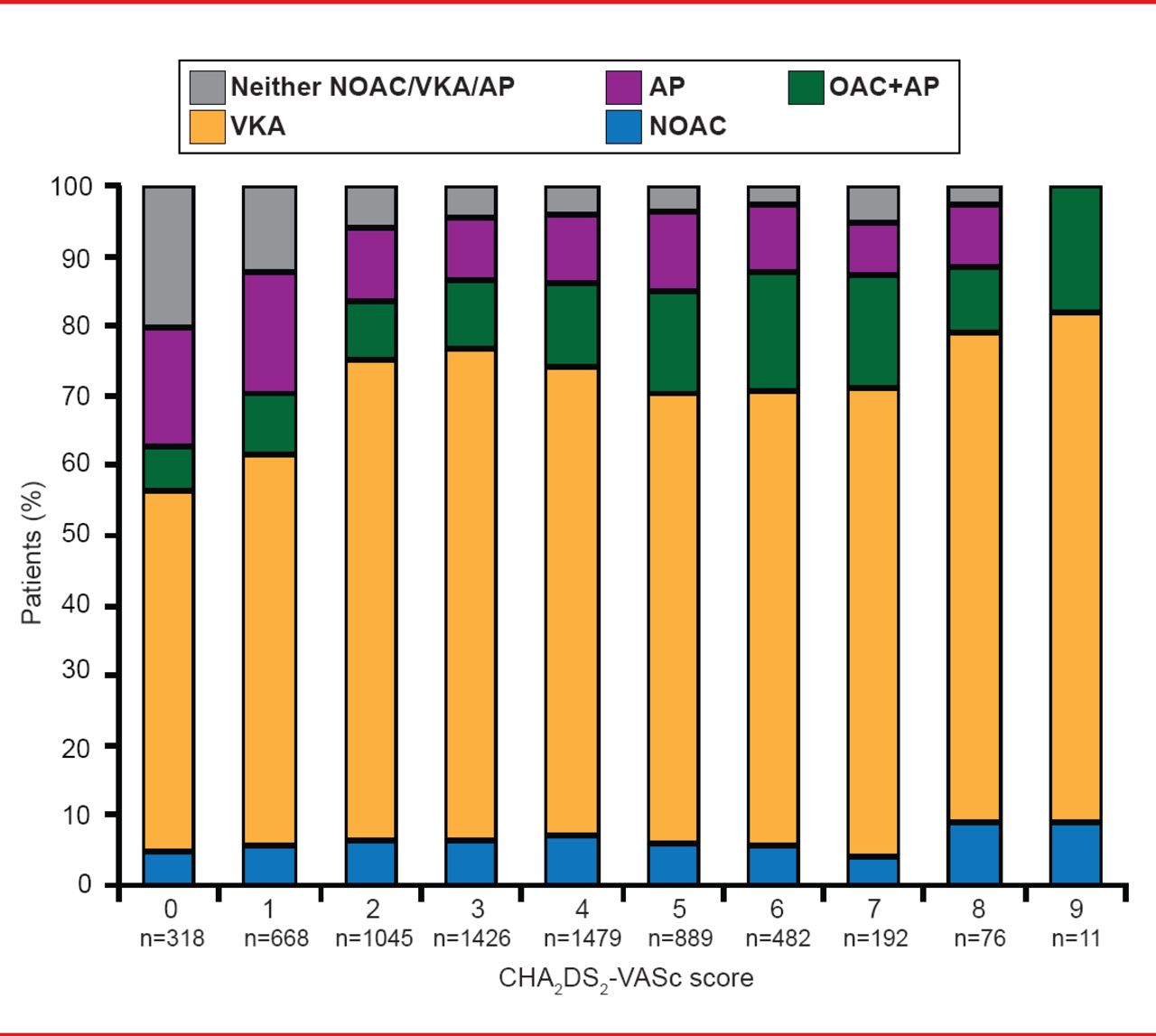
It was also shown that, of patients who were clear-cut candidates for oral anticoagulant drugs (OACs), >80% actually received therapy in accordance with recommended guidelines. Most received vitamin K antagonists (VKAs) as monotherapy, although others received antiplatelet (AP) monotherapy, combined OACs and AP, or new OACs (Figure 2).

Type of Antithrombotic Therapy Used
AP=antiplatelet; NOAC=new oral anticoagulant; OAC=oral anticoagulant; VKA=vitamin K antagonists.
Reproduced with permission from P Kirchhof, MD.
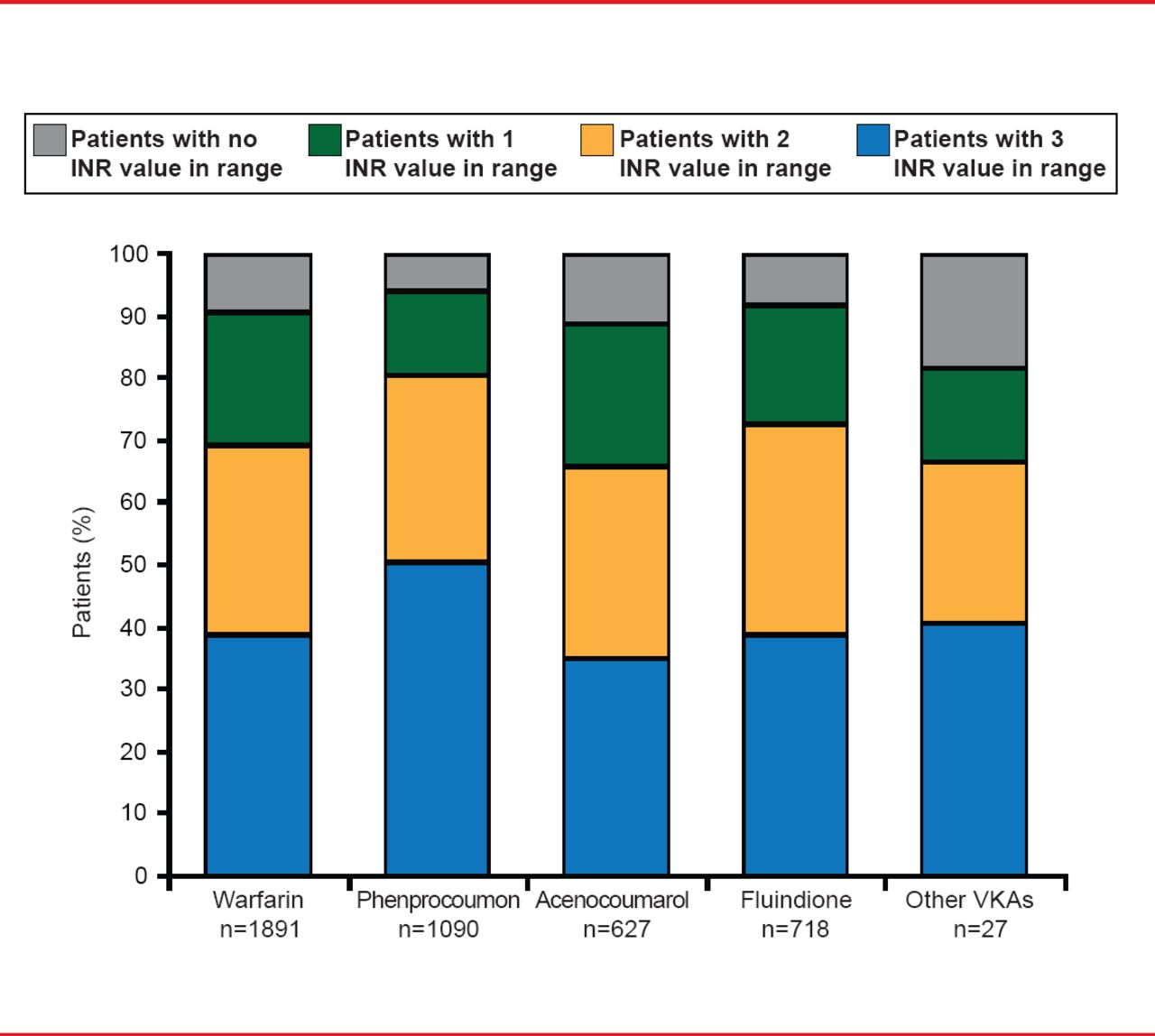
Anticoagulation management by VKAs was also evaluated, based on 3 international normalized ratio (INR) values collected at baseline visit. Approximately two thirds of patients showed adequate anticoagulant control, having 2 out of 3 INRs within the therapeutic range, and <50% had all 3 INR values within the therapeutic range (Figure 3).

Quality of Anticoagulation Control Using VKAs
INR=international normalized ratio; VKA=vitamin Kantagonists.
Reproduced with permission from P Kirchhof, MD.
It was also found that adequate heart rate control (within 60 to 100 bpm) was achieved in most patients with AF. However, more than half of them had a European Heart Rhythm Association score of III to IV, indicating a reduced quality of life due to severe or disabling AF symptoms. And although amiodarone is the form of rhythm control therapy being used most extensively in these patients, AF ablation is also being increasingly used. However, it was also shown that more than half of the most symptomatic patients do not receive rhythm control therapy
The researchers concluded that the baseline data demonstrates a change in clinical practice since the publication of the updated ESC guidelines in 2010 for management of patients with AF. However, although many patients are receiving OAC therapy in accordance with recommended guidelines, many patients remain symptomatic yet still do not receive rate control therapy. Although these findings will need to be confirmed at the 12-month follow-up visit, improved strategies may be necessary to enhance outcomes in patients with AF.
Altogether 78.6% of patients were adequately rate controlled, using a mean heart rate of 60 to 100 bpm as the definition. Rhythm control therapy was given to 66.7% of patients, with rhythm control consisting of electrical cardioversion in 18.1% of patients; pharmacological conversion in 19.5%; amiodarone in 24.1%; flecainide in 10.5%; sotalol in 5.5%; dronedarone in 4%; other antiarrhythmic drugs in 3.1%; and catheter ablation in 5%. However, over 80% of patients still suffered from AF symptoms despite good rate control.
“We were surprised and puzzled by the high number of patients who suffer from AF despite good rate control,” said Prof. Kirchhof. “This indicates that we have more work to do to develop tools to better prevent AF and possibly to better maintain sinus rhythm in the future.”
The ongoing Early Treatment of Atrial Fibrillation for Stroke Prevention Trial [EAST; www.easttrial.org] is currently testing whether early use of rhythm control therapy can prevent adverse cardiovascular outcomes in patients with AF compared with usual care. EAST will help to define whether early rhythm control therapy can improve the management of patients with AF.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.