

Summary
Adrenal insufficiency is a rare disease that is difficult for patients to live with due to the lifelong requirement of steroid therapy and the ever-present risk of adrenal crisis. This article discusses the diagnosis of adrenal insufficiency, prevalence and prevention for adrenal crisis, and recent advances in the treatment of Addison's disease.
- Renal Disease
- Adrenal Disorders
- Renal Disease
- Adrenal Disorders
- Endocrinology
- Diabetes & Metabolic Syndrome
Adrenal insufficiency is a rare disease that is difficult for patients to live with due to the lifelong requirement of steroid therapy and the ever-present risk of adrenal crisis. Kristian Løvås, MD, PhD, Haukeland University Hospital, Bergen, Norway, presented on the diagnosis of adrenal insufficiency, and emphasized the importance of being aware that adrenal insufficiency is possible and that it requires immediate treatment.
Most patients with adrenal insufficiency present with fatigue and weight loss, and may also have hypotension. In addition, hyperpigmentation and salt cravings are highly specific symptoms of primary adrenal insufficiency. If serum cortisol and adrenocorticotropic hormone (ACTH) levels are low, secondary adrenal insufficiency is likely, but additional testing is usually required for a definitive diagnosis. The insulin tolerance test is the gold standard. If ACTH is high, then primary adrenal insufficiency is likely. Prof. Løvås pointed out that an early diagnosis of primary adrenal insufficiency, particularly that caused by an autoimmune disorder, is important but difficult to achieve. Positive 21-hydroxylase (21OH) autoantibodies are associated with a greater risk of autoimmune adrenal insufficiency, particularly in children [Coco G et al. J Clin Endocrinol Metab 2006]. In 21OH-positive individuals, testing the levels of ACTH in the morning is a better predictor than ACTH stimulation testing [Baker P et al. Clin Endocrinol 2012].
Prof. Løvås recommended that one should be aware of unusual phenotypes of autoimmune Addison's disease, such as those which may occur in autoimmune polyendocrine syndrome type 1, which is caused by a mutation in the AIRE gene. Symptoms include hypoparathyroidism, chronic fungal infection, enamel dysplasia, and a young age of onset. A definitive diagnosis can be made by testing for autoantibodies against interferon (IFN)-ω. If the patient is negative for 21OH-antibodies, then computed tomography of the adrenal glands should be performed, which can identify hemorrhage of the adrenals due to Waterhouse-Friderichsen syndrome, anticoagulant therapy, or antiphospholipid syndrome, as well as tuberculosis, or tumors. Another uncommon phenotype is that of adrenoleukodystrophy (ALD), which is caused by a mutation in the ABCD1 gene. Patients with ALD will test negative for IFN-ω and 21OH autoantibodies, but have elevated levels of very long chain fatty acids in serum.
Stephanie Hahner, MD, University Hospital Wuerzburg, Wuerzburg, Germany, discussed the prevalence and prevention for adrenal crisis. In an analysis of 1675 patients with primary adrenal insufficiency, the risk ratio for all-cause mortality in men was 2.19 (95% CI, 1.91 to 2.51) and 2.86 (95% CI, 2.54 to 3.20) in women [Bergthorsdottir R et al. J Clin Endocrinol Metab 2006]. In addition, Addison's disease itself is the second most common cause of death in patients with Addison's disease, with cardiovascular disease first [Erichsen MM et al. Eur J Endocrinol 2009]. Interestingly, patients with Addison's disease are at a greater risk of dying from an infection than the general population, with a risk ratio of 1.74 (95% CI, 0.97 to 2.87) and 3.74 (95% CI, 2.52 to 5.34) in men and women, respectively, for respiratory disease, and 6.57 (95% CI, 2.56 to 15.17) and 5.57 (95% CI, 2.04 to 12.13) in men and women, respectively, for other infectious diseases [Bergthorsdottir R et al. J Clin Endocrinol Metab 2006]. This may relate to inadequate treatment of adrenal crises.
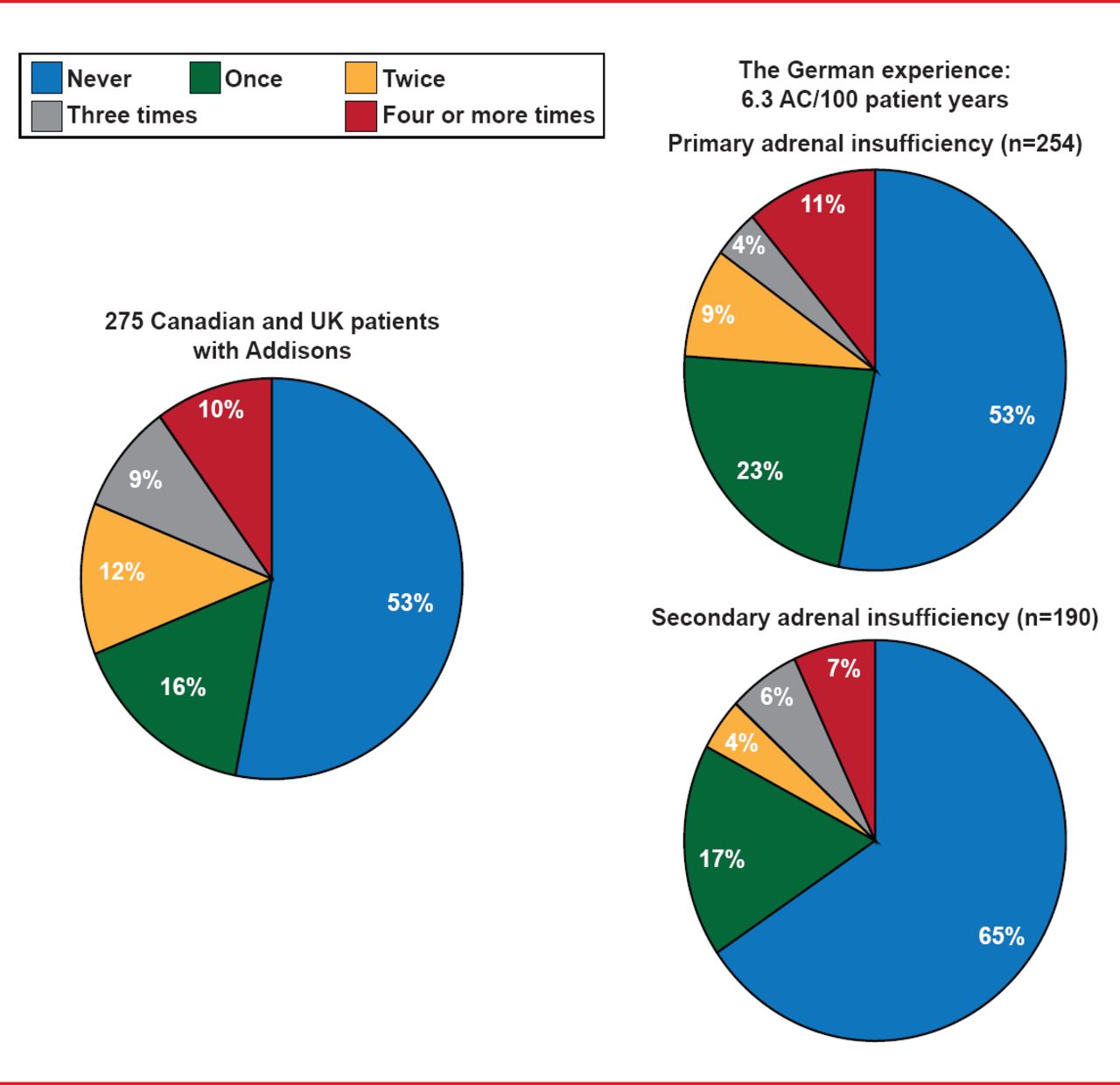
Adrenal crisis is estimated to occur 6.3 times per 100 patient years, with 23% and 17% of German patients with primary and secondary adrenal insufficiency, respectively, having required emergency treatment at least once since their diagnosis (Figure 1) [Hahner S et al. Eur J Endocrinol 2010]. In a study of 275 Canadian and UK patients with Addison's disease, 16% of patients required emergency care once since their diagnosis [White K, Arlt W. Eur J Endocrinol 2010]. A retrospective analysis of 444 patients with adrenal insufficiency only identified limited risk factors for adrenal crisis [Hahner S et al. Eur J Endocrinol 2010].

Incidence of Adrenal Crisis in Patients With Adrenal Insufficiency
Reproduced with persmission from S Hahner, MD.
In a 2-year prospective trial of 455 patients with adrenal insufficiency, adrenal crisis occurred at a rate of 7.8 per 100 patient years. In addition, 2 patients died following hospitalization for adrenal crisis and 2 additional patients died due to adrenal crisis after the study had been completed. Factors preceding adrenal crisis included gastroenteritis, fever or infection, psychological stress, and surgery. Importantly, 30% of patients that entered adrenal crisis experienced no relief of symptoms following oral hydrocortisone; however, intravenous hydrocortisone did result in improvement.
Prof. Hahner highlighted that for the prevention and treatment of adrenal crisis: it is important that patients are able to self-inject glucocorticoids. Patients with adrenal insufficiency should have an emergency card on their person, as well as an emergency set containing hydrocortisone. A study of 12 patients with autoimmune Addison's disease demonstrated that 100 mg of subcutaneous or intramuscular hydrocortisone resulted in a rapid and substantial increase in serum cortisol levels (p=0.004) [Hahner S et al. Eur J Endocrinol 2013]. Prof. Hahner suggested that perhaps a hydrocortisone pen should be produced for patients with adrenal insufficiency to carry in case of adrenal crisis.
Simon H.S. Pearce, MBBS, MD, Newcastle University, Newcastle Upon Tyne, United Kingdom, presented recent advances in the treatment of Addison's disease. Patients with adrenal insufficiency require lifelong treatment with glucocorticoids, but clearly, a cure would be better.
In a small study, 6 patients with primary adrenal failure diagnosed within 28 days were treated with rituximab 1 g on Days 1 and 15 and followed for 1 year [Pearce SH et al. J Clin Endocrinol Metab 2012]. Following rituximab therapy, B lymphocyte levels dropped to undetectable levels for 5 months and the 21OH autoantibodies decreased in the 5 patients who were 21OH autoantibody positive. Cortisol levels decreased rapidly in 5 patients. However, 1 patient experienced an initial decrease in cortisol, but by 6 months her cortisol levels increased to baseline, by 12 months her cortisol levels were back to those at diagnosis, and by 15 months her peak cortisol was over 400 nmol. The patient was able to wean off of hydrocortisone and remained in remission from Addison's disease for 17 months.
Prof. Pearce suggested that administering hydrocortisone to patients with adrenal insufficiency at diagnosis may actually be detrimental to the residual function of their adrenal glands. He noted that in the study of six patients, all experienced a decrease of about two thirds in their cortisol at the study baseline, which was only 2 to 3 weeks after their initial diagnosis and cortisol level measurements. Because the adrenal progenitor cells do not normally express 21OH, they may be intact despite the presence of Addison's [Wood MA, Hammer GD. Mol Cell Endocrinol 2011].
In the Revival of Stem Cells in Addison's Study [RoSA; NCT01371526] study, 13 patients with Addison's disease for at least 1 year and up to 19 years received 1 mg of tetracosactrin subcutaneous injections on alternate days for up to 20 weeks. Two patients experienced a dramatic increase in cortisol levels and eventually experienced remission from Addison's disease, with 1 still in remission and the other requiring steroid therapy after about 6 months of remission. All patients treated with tetracosactrin therapy experienced hyperpigmentation and 4 out 9 premenopausal women had menstrual disturbances. Prof. Pearce concluded by suggesting that some patients with Addison's disease have residual adrenal function, which may be remediable.
Traditionally, adrenal insufficiency has been treated with glucocorticoid therapy. Although more research is needed, recent studies demonstrate that new therapies with the potential for eliciting remission may be on the horizon.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.