

Summary
The past decades have demonstrated significant improvements in the care and resulting outcomes of patients presenting with an acute coronary syndrome (ACS). This article discusses some of the differences between the development of coronary disease, its clinical presentation, and the outcomes between men and women.
- Myocardial Infarction
- Prevention & Screening
- Coronary Artery Disease
- Myocardial Infarction
- Cardiology & Cardiovascular Medicine
- Prevention & Screening
- Coronary Artery Disease
The past decades have demonstrated significant improvements in the care and resulting outcomes of patients presenting with an acute coronary syndrome (ACS). In her presentation, Angela Maas, MD, PhD, University Medical Center in St Radboud, Nijmegen, The Netherlands, highlighted some of the differences between the development of coronary disease, its clinical presentation, and the outcomes between men and women. For example, a well-described phenomenon is that women presenting with ST-elevation myocardial infarction are more than twice as likely to have “nonobstructive” coronary epicardial disease compared with men, yet higher mortality [Anderson RD et al. Circulation 2007].
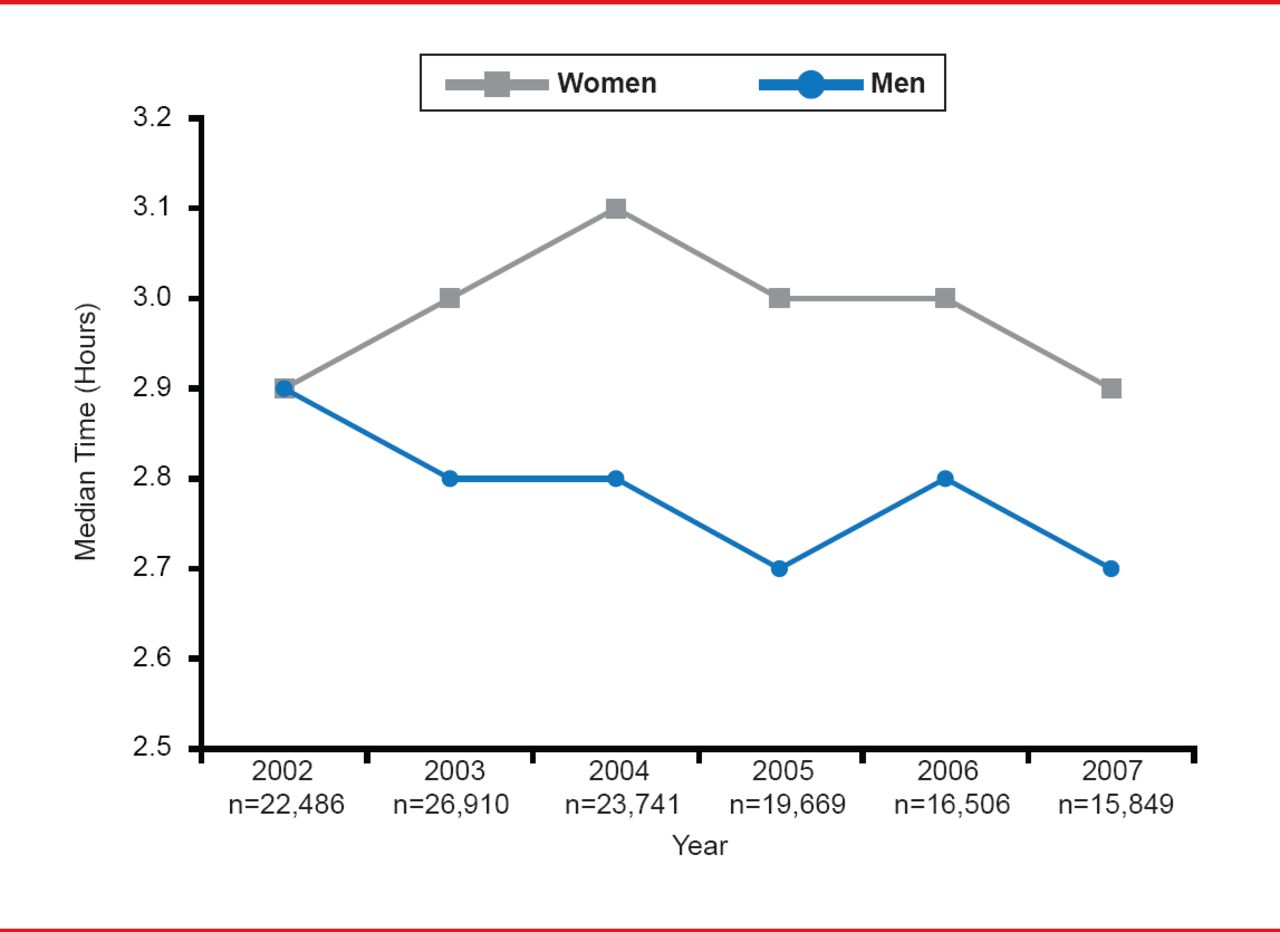
One possible cause of higher mortality rate in women might be a longer time from symptom onset to hospital presentation, perhaps because the impact of cardiovascular disease is often underappreciated by women and the presence of “atypical” symptoms may obscure the true etiology. For instance, 37% of women present without pain during an ACS, compared with only 27% of men [Canto JG et al. Arch Intern Med 2007]. Other symptoms in women could include difficulty breathing, flu symptoms, fatigue, anxiety or loss of appetite. Studies in the past decade have found that women usually present 17 to 20 minutes later than men when having an MI (Figure 1) [Kaul P et al. Am Heart J 2011; Diercks DB et al. Am Heart J 2010]. Consideration of alternative diagnoses in women is also critical, especially coronary dissection in those aged <60 years and stress-induced cardiomyopathy depending upon the presentation [Mackman N. Nature 2008].
Physicians should also be aware that mortality is higher in women despite better TIMI flow at the time of the patient's first angiography and less multi-vessel disease [Otten AM et al. Eur Heart J Acute Cardiovasc Care 2013]; perhaps related to more vasospasm during an acute MI [Thygesen K et al. J Am Coll Cardiol 2012]. Study of women with unstable and stable coronary disease has revealed that women have less calcification, more often diffuse epicardial disease without discrete luminal narrowing, and significant involvement of the coronary microvasculature circulation [Reynolds HR et al. Circulation 2011]. In contrast to men, women with ACS may have other exacerbating factors such as estrogen deficiency, and are more likely to have metabolic syndrome and diastolic dysfunction [Pizzi C, Bugiardini R. Heart 2010].

Women Delay Presenting to Hospital With MI
Reproduced from Diercks B et al. Gender differences in time to presentation for myocardial infarction before and after a national women's cardiovascular awareness campaign: A temporal analysis from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress ADverse Outcomes with Early Implementation (CRUSADE) and the National Cardiovascular Data Registry Acute Coronary Treatment and Intervention Outcomes Network–Get with the Guidelines (NCDR ACTION Registry–GWTG). Am Heart J 2010;160(1):80. With permission from Elsevier.
A lower rate of obstructive atherosclerosis may have implications when diagnostic testing in women for cardiovascular disease [Shaw LJ et al. J Am Coll Cardiol 2009; Circ Cardiovasc Imaging 2010]. Exercise or bicycle testing, for example, is less useful in diagnosing women due to lower rates of obstructive epicardial disease [Montalescot G et al. Eur Heart J 2013]. Dr. Maas suggested use of coronary flow measurements during catheterization for diagnosis of diffuse obstructive atherosclerosis and computed tomography angiogram in the emergency room for diagnosis of ACS [Troung QA et al. Circulation 2013].
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.