

Summary
This article discusses the use of ventricular assist devices (VADs) and heart transplantation in heart failure patients.
- Interventional Techniques & Devices
- Heart Failure
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Heart Failure
Edward B. Savage MD, Cleveland Clinic Florida, Weston, Florida, USA, discussed the use of ventricular assist devices (VADs) and heart transplantation in heart failure patients.
Dr. Savage emphasized that the type of VAD selected may be in part determined by the patient's likelihood of recovery of cardiac function and the anticipated duration of need for VAD therapy. For example, if short-term therapy is anticipated, an intra-aortic balloon pump, the Impella device, the TandemHeart device, or extracorporeal membrane oxygenation could be used; however, these therapies are less suited to long-term outpatient use. The degree of cardiac support needed, the availability and experience of the physician team, and patient characteristics (eg, size of patient, pulmonary function) are also determinants for which device is selected.
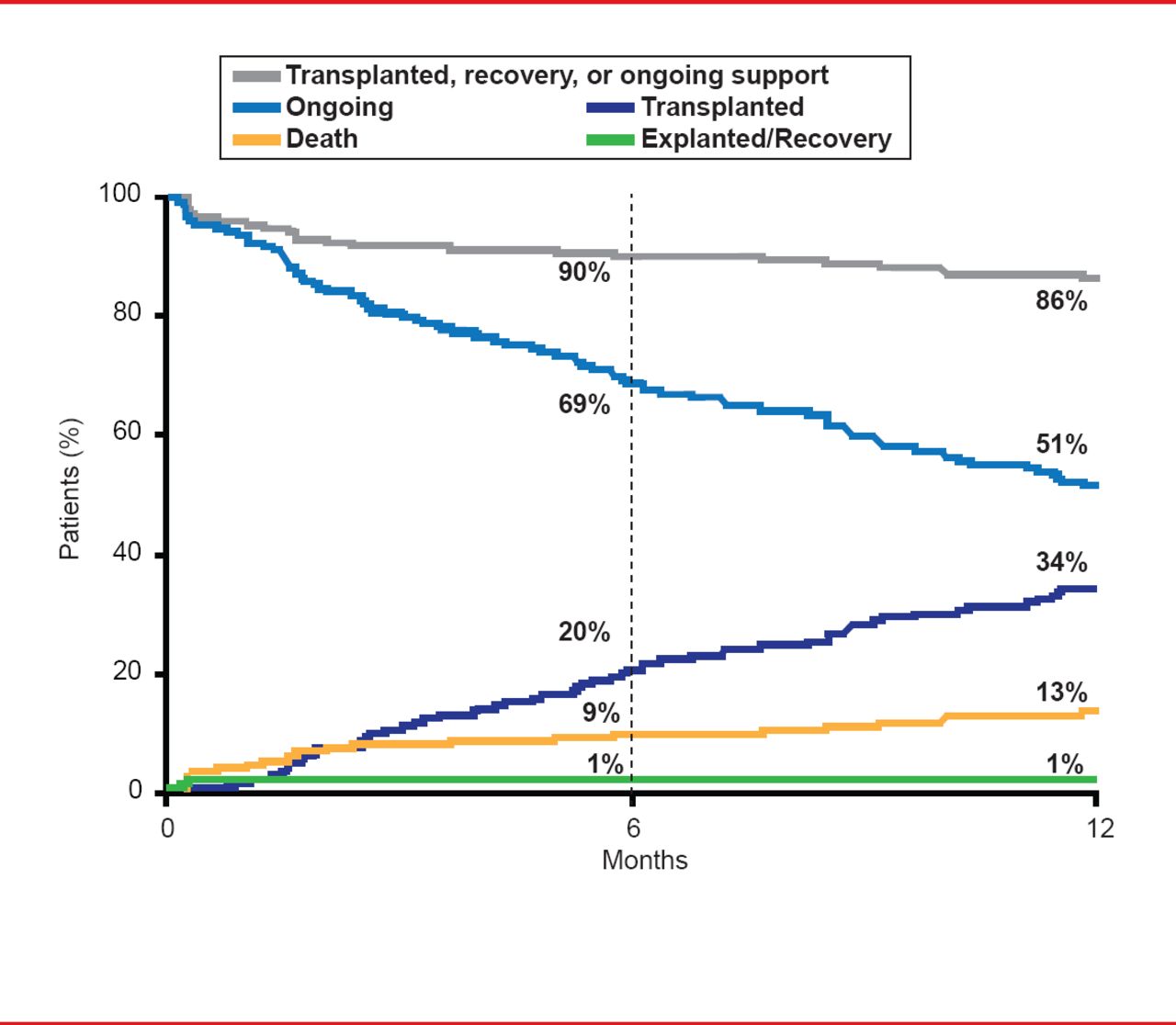
For patients who require long-term cardiac support, implantable devices include the Syncardia's Cardiowest total artificial heart; the Heartware ventricular assist system; and Thoratec's HeartMate II (HM II) left VAD (LVAD). As one example, the HM II can be used as an LVAD and is approved as a bridge to heart transplant as well as destination therapy (ie, no heart transplant planned). Data from a postmarket approval study of the first 169 patients enrolled in the Interagency Registry for Mechanically Assisted Circulatory Support [INTERMACS], was consistent with the improved outcomes seen in prior clinical trial data. At 12 months, the survival rate for patients remaining on HM II LVAD support was 86%, compared with only 70% for patients with other types of LVADs (p<0.001; Figure 1) [Starling RC et al. J Am Coll Cardiol 2011].

12-Month Outcomes for HM II LVAD Bridge to Transplant
Reproduced from Starling RC et al. Results of the Post-U.S. Food and Drug Administration-Approval Study With a Continuous Flow Left Ventricular Assist Device as a Bridge to Heart Transplantation. J Am Coll Cardiol 2011;57(19):1890–1898. With permission from Elsevier.
Dr. Savage reviewed the progress in heart transplantation since 1967. Advancements in immunosuppressive therapy in conjunction with improvements in surgical technique, organ harvesting/preservation, patient selection, and other factors have been the primary reason for continued improvements in patient prognosis. Data on the current characteristics and survival of patients post transplant from the 2011 annual report of the Scientific Registry of Transplant Recipients (SRTR) and Organ Procurement and Transplantation Network (OPTN) were discussed [OPTN and SRTR. OPTN/SRTR 2011 Annual Data Report. Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation; 2012. Available at http://srtr.transplant.hrsa.gov/annual_reports/2011/flash/05_heart/index.html]. Dr. Savage mentioned factors associated with reduced waiting times for heart transplant including 1) United Network for Organ Sharing Status 1A or 1B; 2) VAD implantation; and 3) blood type A, B, or AB. Dr. Savage noted that it tends to be more difficult to find a match for patients with type O blood, since they can only receive a heart from a type O donor. The majority of transplanted adults continued to be males and the mean age at transplantation in 2011 was 50.9 years. Coronary artery disease as an etiology of cardiac failure in this population appears to be decreasing while nonischemic cardiomyopathies is increasing.
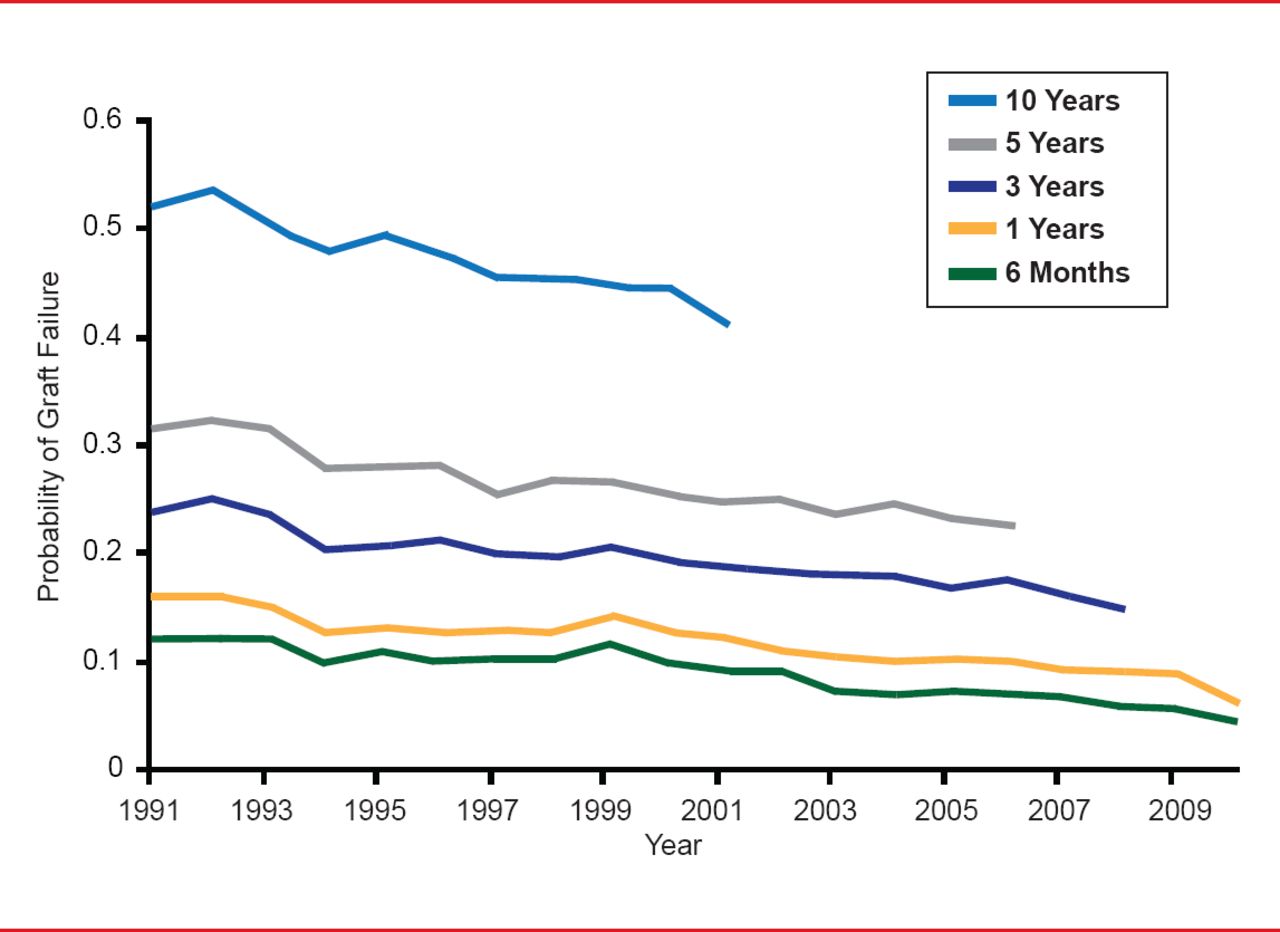
Dr. Savage concluded by highlighting that although the total annual number of heart transplants performed in the United States remains steady (∼1800 to 2000), based on availability of donor hearts, the rate of survival to first graft failure in recipients continues to improve (Figure 2) [OPTN and SRTR. OPTN/SRTR 2011 Annual Data Report. HHS/HRSA/HSB/DOT 2012. Available at http://srtr.transplant.hrsa.gov/annual_reports/2011/flash/05_heart/index.html].

Decreasing Acute and Long-Term Graft Failure
Source: OPTN and SRTR. OPTN/SRTR 2011 Annual Data Report.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.