

Summary
Selecting the right antidiabetic therapy for patients with heart failure (HF) and type 2 diabetes mellitus (T2DM) can be challenging. This article reviewed approaches to managing dysglycemia in patients with HF, including intensive versus less intensive control and treatments.
- Heart Failure
- Hyperglycemia/Hypoglycemia
- Diabetes Mellitus
- Heart Failure
- Hyperglycemia/Hypoglycemia
- Diabetes Mellitus
- Endocrinology
- Diabetes & Metabolic Syndrome
Selecting the right antidiabetic therapy for patients with heart failure (HF) and type 2 diabetes mellitus (T2DM) can be challenging. Miles Fisher, MD, Glasgow Royal Infirmary, Glasgow, United Kingdom, reviewed approaches to managing dysglycemiain patients with HF.
INTENSIVE VERSUS LESS INTENSIVE CONTROL
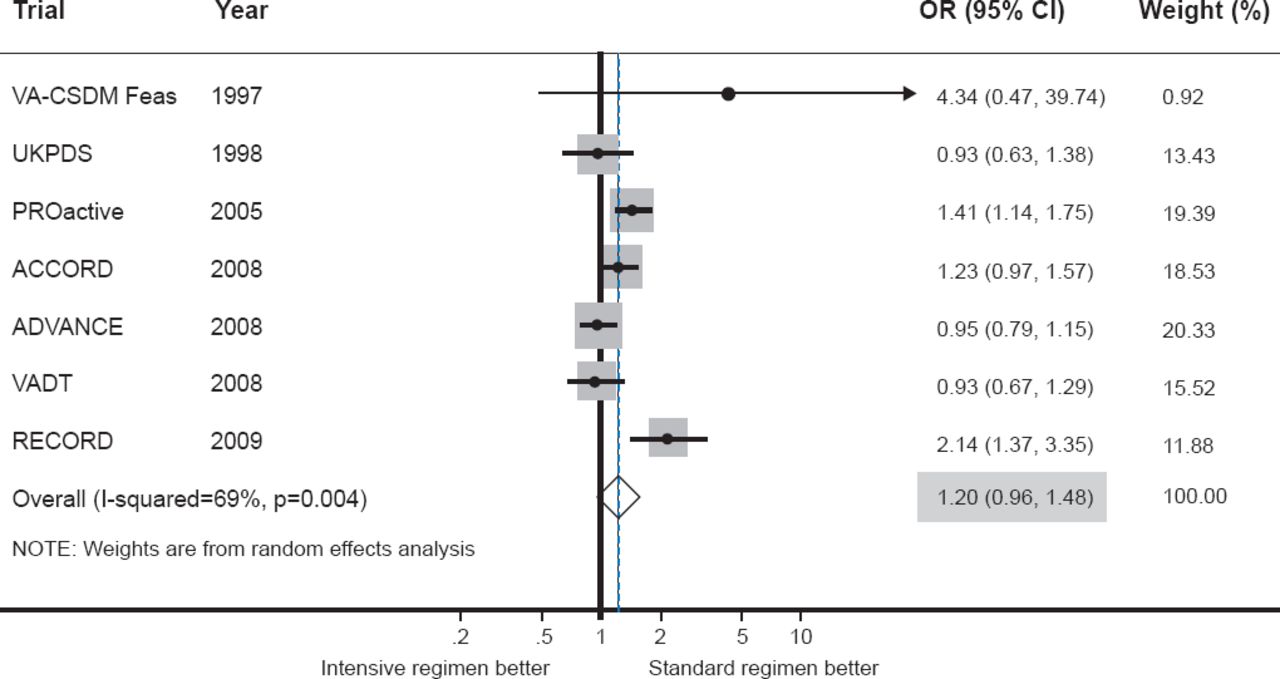
To-date the data remain questionable regarding the prevention of HF by managing dysglycemia. A meta-analysis of eight randomized controlled trials comparing more versus less intensive glucose lowering in patients with T2DM reported that a more intensive control strategy did not reduce the occurrence of HF (OR, 1.20; 95% CI, 0.96 to 1.48; Figure 1) [Castagno D et al. Am Heart J 2011]. Although randomized controlled trial data are scarce for this population of patients, in general, hyperglycemia in patients with T2DM should be treated to appropriate guideline-recommended targets and hypoglycemia should be avoided [Gitt AK et al. Eur J Heart Fail 2012]. Near-normal glycemic targets should be the standard for younger patients with relatively recent onset of T2DM and little or no micro- or macrovascular complications, while somewhat higher targets should be considered for older patients with long-standing diabetes and evidence of cardiovascular disease [Ismail-Beigi F et al. Ann Intern Med 2011].

Intensive Versus Less Intensive Glycemic Control
Reproduced from Castagno D et al. Intensive glycemic control has no impact on the risk of heart failure in type 2 diabetic patients: Evidence from a 37,229 patient meta-analysis. Am Heart J 2011;162(5):938-942. With permission from Elsevier.
TREATMENTS
In a case-control study of patients with T2DM and HF matched for age, sex, clinic site, calendar year, and duration of follow-up, only metformin monotherapy (OR, 0.65; 95% CI, 0.48 to 0.87) or metformin in combination with other drugs (OR, 0.72; 95% CI, 0.59 to 0.90) was associated with reduced HF-related mortality compared with diabetic patients who were not exposed to antidiabetic drugs [MacDonald MR et al. Diabetes Care 2010].
A systematic review and meta-analysis of the seven randomized double-blind clinical trials of drug-related congestive HF in diabetic patients given thiazolidinediones (either rosiglitazone or pioglitazone) showed these agents increased the risk of developing congestive HF across a wide background of cardiac risk (RR, 1.72; 95% CI, 1.21 to 2.42; p=0.002) [Lago RM et al. Lancet 2007].
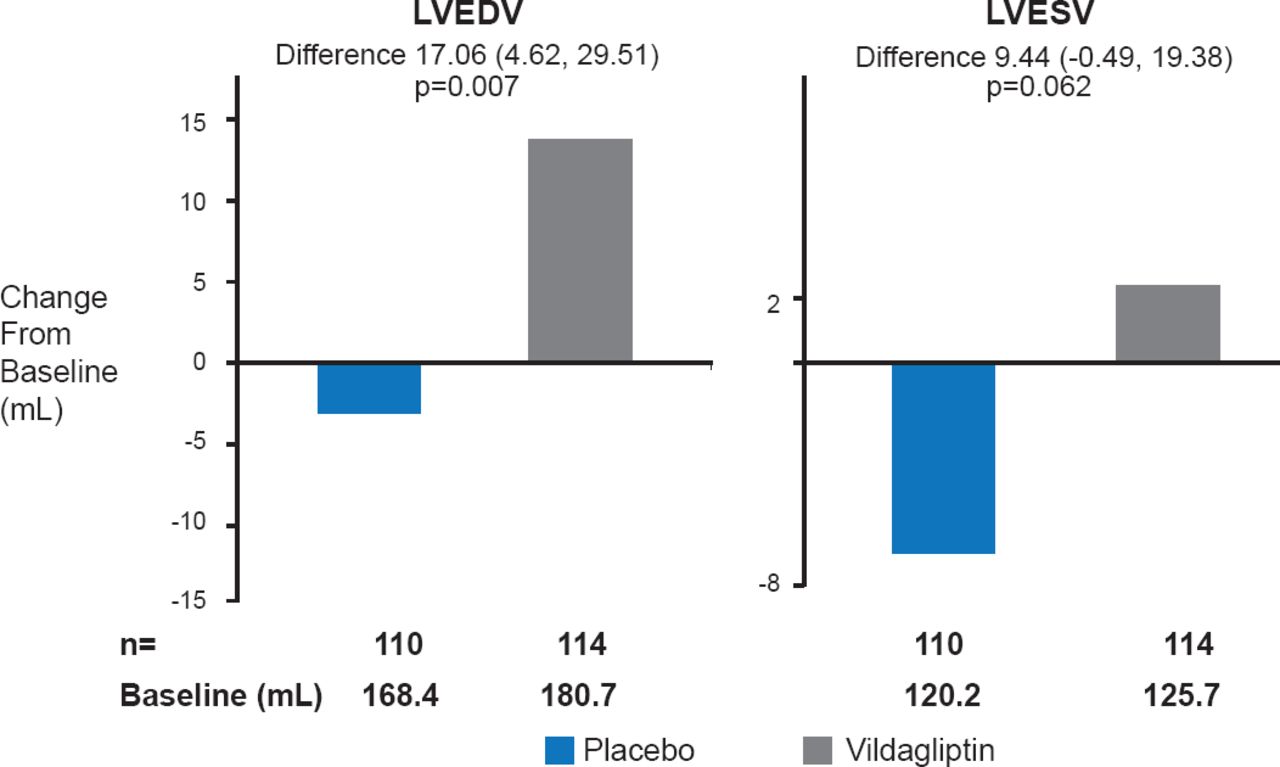
The SGLT2 inhibitors may offer benefits in terms of fluid volume reduction, but it is just as possible that they may cause additional harm in terms of volume depletion in vulnerable patients. In very recent trial, vildagliptin was shown to have glycemic benefit in patients with T2DM and HF but its cardiovascular safety remains unclear. Although there was no difference in left ventricular ejection fraction compared with placebo, there was an unexpected significant increase in left ventricular end-diastolic volume and a nonsignificant increase in left ventricular end-systolic volume in the vildagliptin group (Figure 2) [McMurray J et al. Heart Failure Congress 2013 (abstr 99)]. According to Prof. Fisher, use of DPP-4 and SGLT2 inhibitors remains questionable until more HF patients are included in randomized controlled trials.

Change in Left Ventricular Volumes
LVEDV=left ventricular end-diastolic volume; LVESV=left ventricular end-systolic volume.
Source: McMurray J et al. Heart Failure Congress 2013 (abstr 990).
Injected antidiabetic drugs, such as glucagon-like peptide-1 (GLP-1), may offer some benefits, but, as with the other therapies, data are limited. GLP-1s preserve cardiac function and structure, decrease inflammation, improve glucose metabolism, increase weight loss, reduce blood pressure, and reduce atherosclerotic lesions. Trials are ongoing with these agents.
Prof. Fisher concluded that among the antidiabetic therapies, metformin is probably safe for patients with diabetes and HF while the glitazones are not and the DPP-4 inhibitors are also possibly unsafe. As for the SGLT2 inhibitors and GLP-1 receptor agonists, it is too soon to tell.
- © 2013 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.