

Summary
The risk of developing major cardiovascular or cerebrovascular events following percutaneous coronary intervention or coronary artery bypass grafting is greater in insulin-treated diabetes mellitus (ITDM) patients compared with diabetes mellitus patients not treated with insulin (non-ITDM). This article presents data from a subgroup analysis of the Comparison of Two Treatments for Multivessel Artery Disease in Individuals With Diabetes trial [FREEDOM; Farkouh ME et al. N Engl J Med 2012].
- Cardiology Clinical Trials
- Coronary Artery Disease
- Diabetes Mellitus
- Interventional Techniques & Devices
- Cardiology Clinical Trials
- Cardiology & Cardiovascular Medicine
- Coronary Artery Disease
- Diabetes Mellitus
- Interventional Techniques & Devices
The risk of developing major cardiovascular or cerebrovascular events (MACCE) following percutaneous coronary intervention (PCI) or coronary artery bypass grafting (CABG) is greater in insulin-treated diabetes mellitus (ITDM) patients compared with diabetes mellitus patients not treated with insulin (non-ITDM). George D. Dangas, MD, PhD, Mount Sinai Hospital, New York, New York, USA, presented data from a subgroup analysis of the Comparison of Two Treatments for Multivessel Artery Disease in Individuals With Diabetes trial [FREEDOM; Farkouh ME et al. N Engl J Med 2012].
Diabetes mellitus is currently estimated to affect 6.4% of the worldwide population and is expected to increase in prevalence to 7.7% by 2030. In the United States, ∼26% of patients have ITDM and these patients are at a greater risk of experiencing a cardiovascular (CV) event after PCI, as well as developing wound infections and death following CABG. The purpose of the FREEDOM trial was to evaluate the best method of revascularization (PCI vs CABG) for patients with diabetes who have multivessel coronary artery disease.
Out of 1900 subjects with diabetes enrolled in the FREEDOM trial, 1850 underwent revascularization. The majority of patients were not receiving insulin (non-ITDM, n=1248) and the remainder were receiving insulin (ITDM, n=602) [Farkouh ME et al. N Engl J Med 2012]. Of the non-ITDM patients, 631 underwent PCI with a drug-eluting stent (DES) and 617 underwent CABG. In the ITDM patients, 325 underwent PCI with a DES and 277 underwent CABG. Many baseline characteristics differed significantly between the non-ITDM and ITDM patients (p≤0.02), with body mass index, duration of diabetes, HbA1C, blood glucose levels on the day of the procedure, blood urea nitrogen, history of hypertension, peripheral neuropathy, congestive heart failure, and acute coronary syndrome greater in the ITDM patients. Non-ITDM patients were older and more likely to have NYHA Class I heart failure when compared with ITDM patients.
In the FREEDOM trial, the composite endpoint of death, stroke, or myocardial infarction (MI) occurred in 29% of patients with ITDM and 19% of patients with non-ITDM (HR, 1.63; 95% CI, 1.32 to 2.02; p<0.001). In addition, ITDM patients were at a greater risk of experiencing 30-day MACCE (HR, 1.54; 95% CI, 1.02 to 2.33; p=0.04) and 1-year MACCE (HR, 1.51; 95% CI, 1.18 to 1.92; p=0.001) when compared with non-ITDM patients.
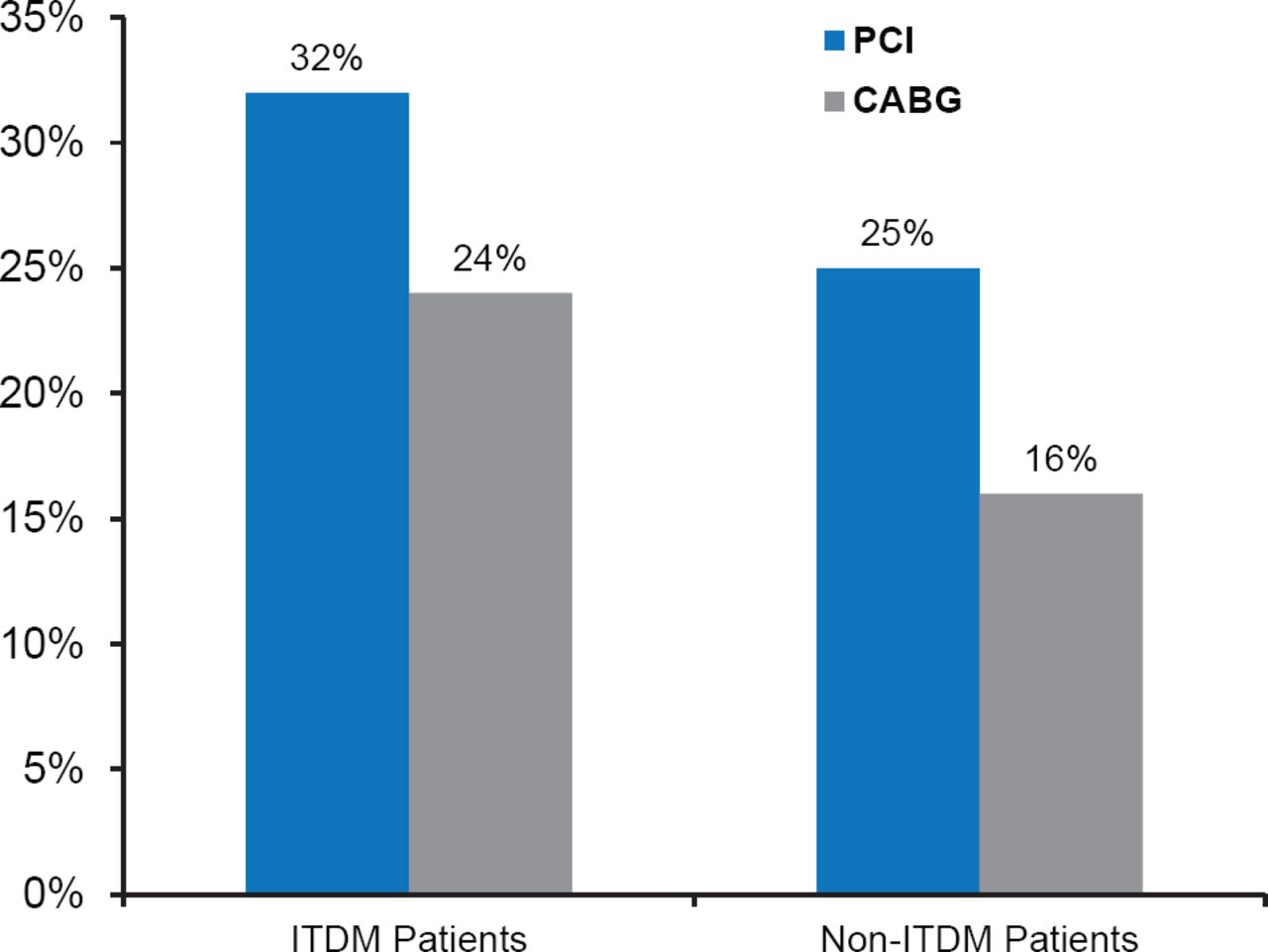
The risk of developing death, stroke, or MI in patients with ITDM was greater following PCI (32%; 95% CI, 26 to 39%) compared with CABG (24%; 95% CI, 19 to 30) at 5 years. A similar trend occurred in patients with non-ITDM, with 25% (95% CI, 19 to 28; Figure 1) of patients experiencing the composite endpoint following PCI compared with 16% (95% CI, 12 to 19) following CABG at 5 years. Risk of death, stroke, or MI was greater in patients with ITDM than in patients with non-ITDM.

Death, Stroke, or MI Following PCI or CABG
CABG=coronary artery bypass grafting; ITDM=insulin-treated diabetes mellitus; PCI=percutaneous coronary intervention.
Dr. Dangas concluded that data from this subanalysis of the FREEDOM trial suggest that ITDM patients experience more MACCE events than non-ITDM patients. However, there was a greater risk of MACCE in patients following PCI compared with CABG regardless of insulin treatment. In addition, Dr. Dangas pointed out that limitations of the study included the lack of randomization of ITDM versus non-ITDM patients, and that the differences in outcomes between patients with ITDM and non-ITDM could be attributed to residual confounding, insulin resistance, or side effects of insulin therapy.
- © 2013 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.