

Article Figures & Data
Figures
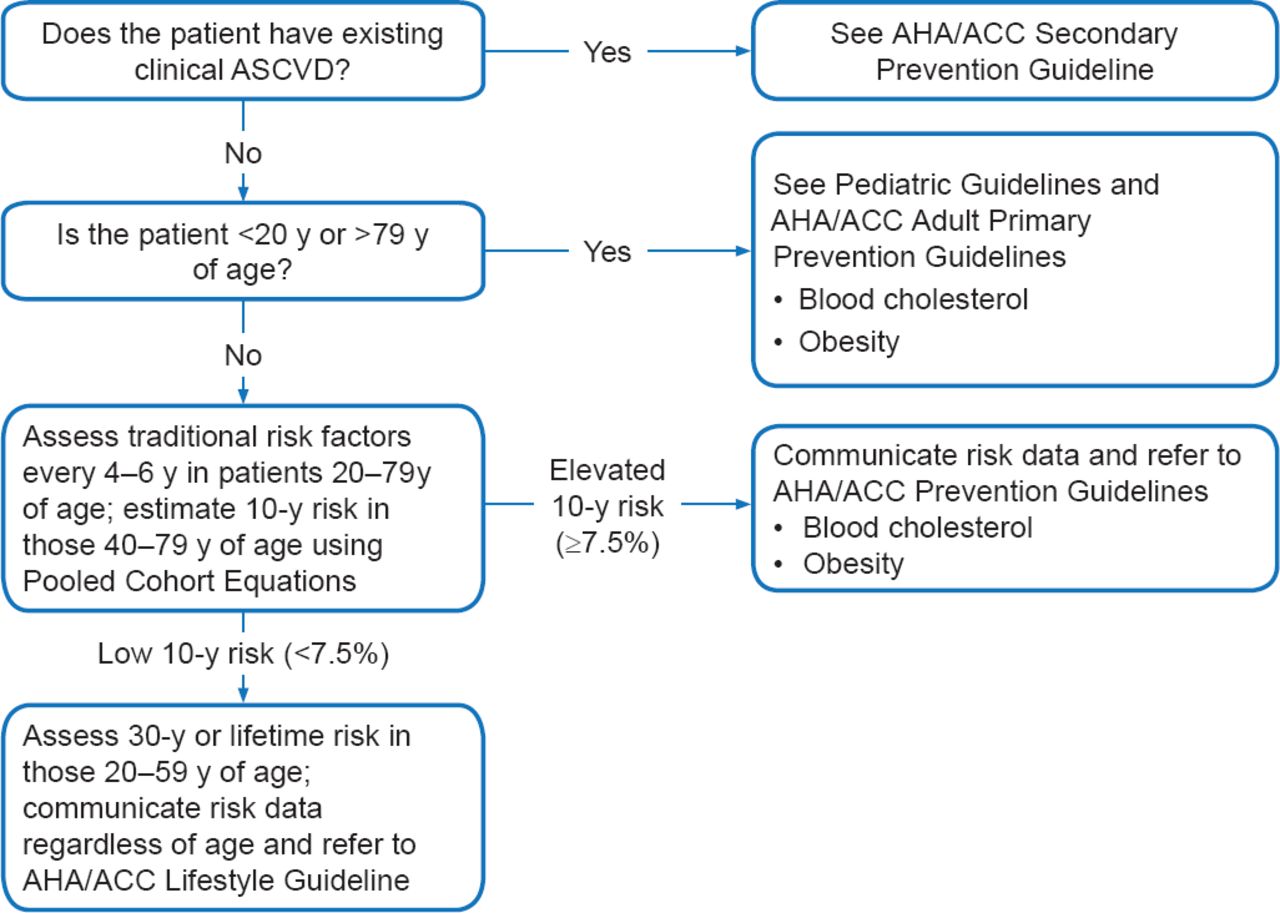
- Figure 1.
Implementation of Risk Assessment Work Group Recommendations
ACC=American College of Cardiology; AHA=American Heart Association; ASCVD=atherosclerotic cardiovascular disease; BMI=body mass index.
Reproduced from Goff DC, Jr et al. ACC/AHA Guideline on the Assessment of Cardiovascular Risk: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
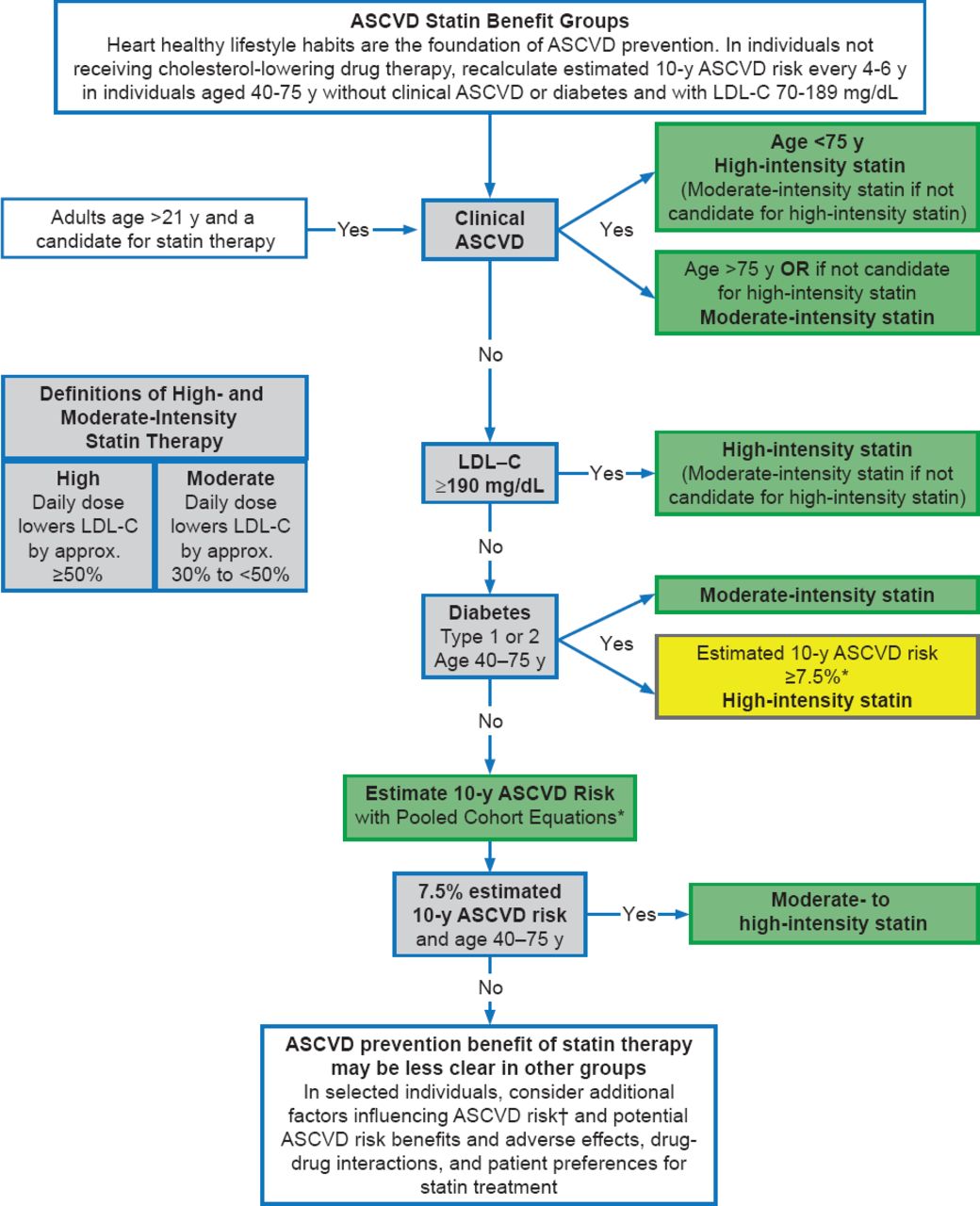
- Figure 2.
Major Recommendations for Statin Therapy for ASCVD Prevention
Colors correspond to the class of recommendations in the ACC/AHA Table 1. This flow diagram is intended to serve as an easy reference guide summarizing recommendations for ASCVD risk assessment and treatment. Assessment of the potential for benefit and risk from statin therapy for ASCVD prevention provides the framework for clinical decision making incorporating patient preferences.
*Percent reduction in LDL-C can be used as an indication of response and adherence to therapy, but is not in itself a treatment goal.
†Primary LDL-C ≥160 mg/dL or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, high-sensitivity C-reactive protein >2 mg/L, CAC score ≥300 Agatston units or ≥75 percentile for age, sex, and ethnicity, ankle-brachial index <0.9, or elevated lifetime risk of ASCVD
ASCVD=atherosclerotic cardiovascular disease; CAC=coronary artery calcium; LDL-C=low-density lipoprotein cholesterol; y=year(s).
Reproduced from Stone NJ et al. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
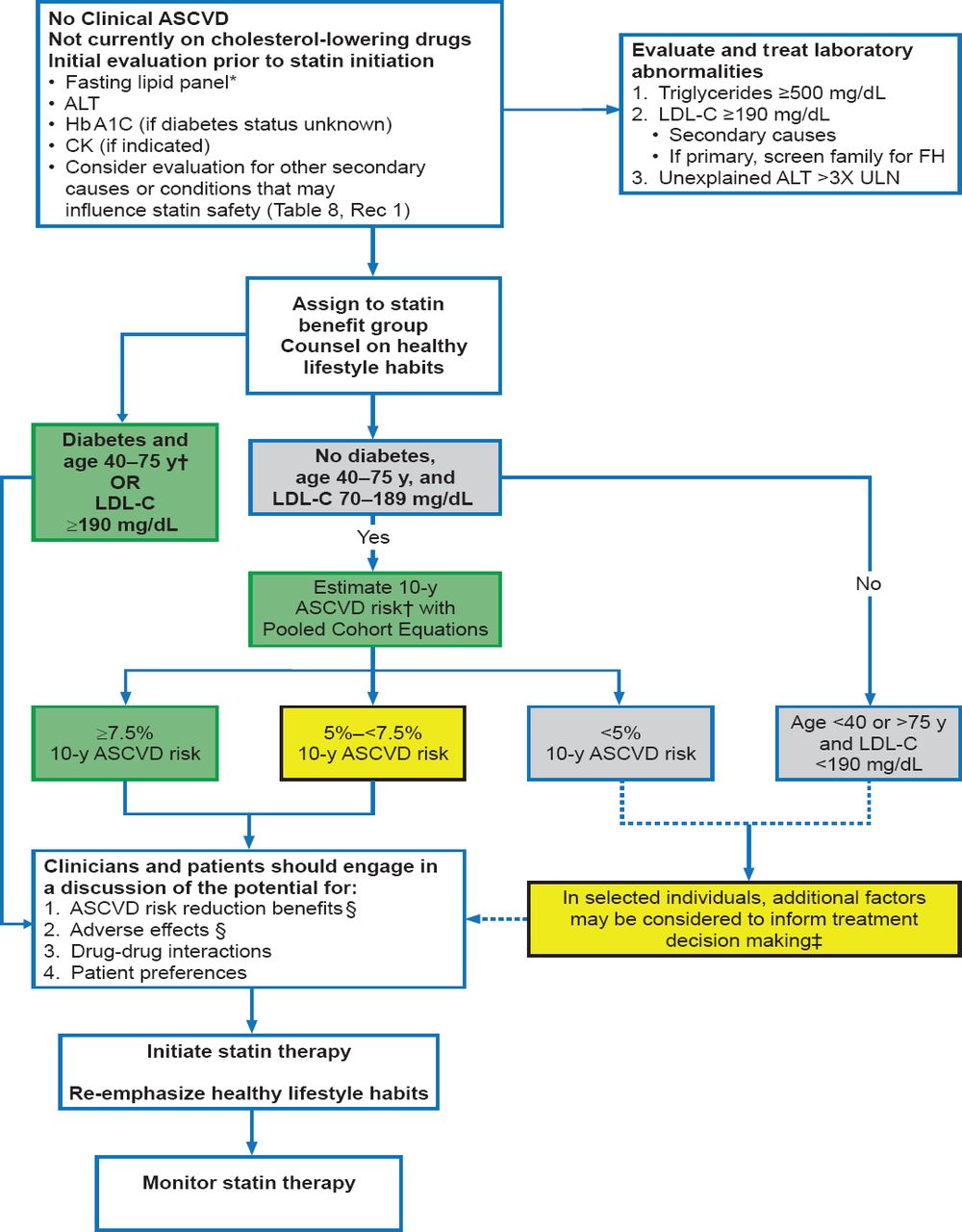
- Figure 3.
Primary Prevention: Initiating Statin Therapy
Colors correspond to the class of recommendations in the ACC/AHA Table 1.
*Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-HDL-C >220 mg/dL may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dL, a fasting lipid panel is required.
†The Pooled Cohort Equations can be used to estimate 10-year ASCVD risk in individuals with and without diabetes.
A downloadable spreadsheet enabling estimation of 10-year and lifetime risk for ASCVD and a web-based calculator are available at http://my.americanheart.org/cvriskcalculator and http://www.cardiosource.org/science-and-quality/practice-guidelines-and-quality-standards/2013-prevention-guideline-tools.aspx.
‡These factors may include primary LDL-C >160 mg/dL or other evidence of genetic hyperlipidemias, family history of premature ASCVD with onset <55 years of age in a first degree male relative or <65 years of age in a first degree female relative, sensitivity-C-reactive protein >2 mg/L ≥300 Agatston units or ≥75 percentile for age, sex, and ethnicity (For additional information, see http://www.mesa-nhlbi.org/CACReference.aspx), ABI <0.9, or lifetime risk of ASCVD. Additional factors that may aid in individual risk assessment may be identified in the future.
§1) Potential ASCVD risk reduction benefits (e.g., absolute risk reduction from moderate- or high-intensity statin therapy can be approximated by using the estimated 10-year ASCVD risk and the relative risk reduction of ∼30% for moderate-intensity statin or ∼45% for high-intensity statin therapy. 2) Potential adverse effects. The excess risk of diabetes is the main consideration in ∼0.1 excess case per 100 individuals treated with a moderate-intensity statin for 1 year and ∼0.3 excess cases per 100 individuals treated with a high-intensity statin treated patients for 1 year. Note: a case of diabetes is not considered equivalent to a fatal or nonfatal MI or stroke. Both statin-treated and placebo-treated participants experienced the same rate of muscle symptoms. The actual rate of statin-related muscle symptoms in the clinical population is unclear. Muscle symptoms attributed to statin should be evaluated in Table 8, Safety Rec 8.
ABI=ankle-brachial index; ALT=alanine transaminase; ASCVD=atherosclerotic cardiovascular disease; CK=creatine kinase; FH=familial hypercholesterolemia; LDL-C=low-density lipoprotein cholesterol; ULN=upper limit of normal.
Editor's Note: All references to other figures and tables within this image refer to items in the original published guidelines as cited below.
Reproduced from Stone NJ et al. ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
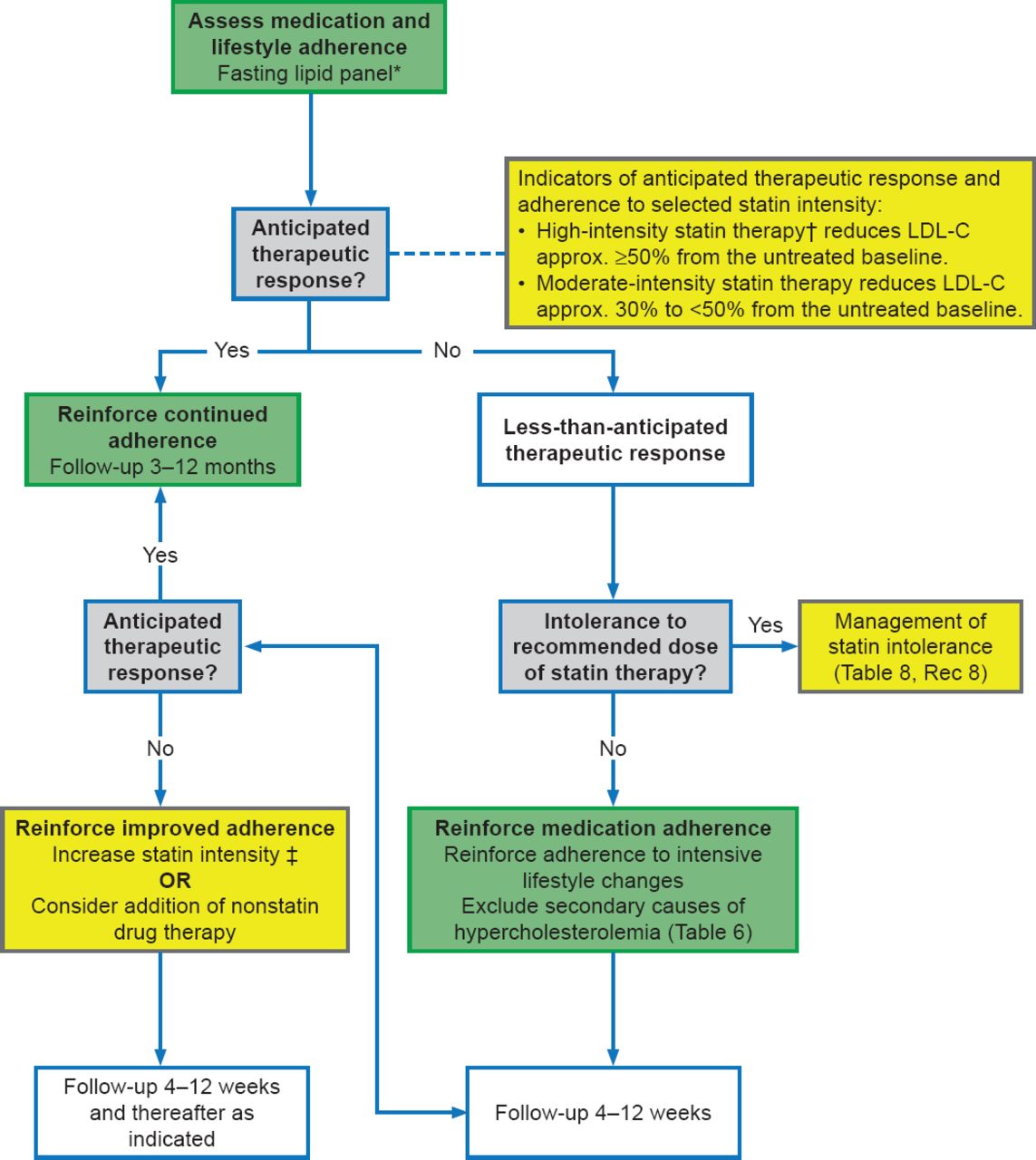
- Figure 4.
Statin Therapy: Monitoring Response and Adherence
Colors correspond to the class of recommendations in the ACC/AHA Table 1.
*Fasting lipid panel preferred. In a nonfasting individual, a nonfasting non-HDL-C >220 mg/dL may indicate genetic hypercholesterolemia that requires further evaluation or a secondary etiology. If nonfasting triglycerides are >500 mg/dL, a fasting lipid panel is required.
†In those already on a statin, in whom baseline LDL-C is unknown, an LDL-C <100 mg/dL was observed in most individuals receiving high-intensity statin therapy in RCTs.
‡In those already on a statin, in whom the baseline LDL-C is unknown, an LDL-C <100 mg/dL was observed in most individuals receiving high-intensity statin therapy in RCTs. For further review see Section 6.3.1 of the guidelines.
ASCVD=atherosclerotic cardiovascular disease; HDL-C=high-density lipoprotein cholesterol; LDL-C=low-density lipoprotein cholesterol; RCT=randomized clinical trial
Editor's Note: All references to other figures and tables within this image refer to items in the original published guidelines as cited below.
Reproduced from Stone NJ et al. 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2013. With permission from Lippincott, Williams and Wilkins.
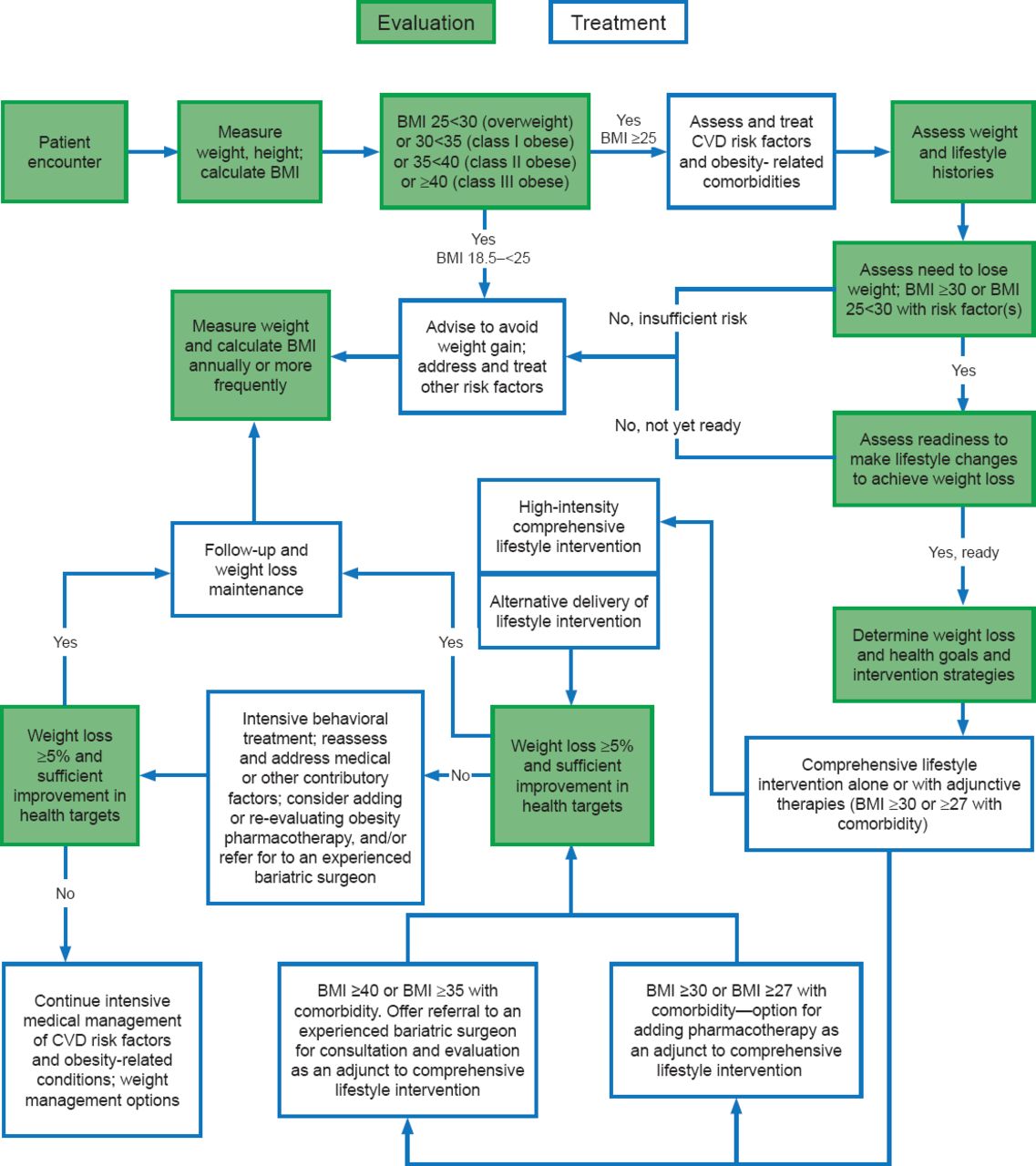
- Figure 5.
Chronic Care Model of Weight Management by Primary Care Providers
BMI=body mass index; CVD=cardiovascular disease; FDA=Food and Drug Administration.
†BMI cut-point determined by the FDA and listed on the package inserts of FDA-approved obesity medications.
Editor's Note: This algorithm applies to the assessment of overweight and obesity in adults and subsequent decisions based on that assessment. Each step (designated by a box) in this process is reviewed in this section and expanded upon in subsequent sections within the original guidelines article as cited below.
Reproduced from Jensen MD et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society. Circulation 2013. With permission from Lippincott, Williams and Wilkins.





Tools
Guidelines for Prevention of Atherosclerotic Cardiovascular Disease
Permalink:









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.