

Summary
A recent meta-analysis reported that delayed thrombosis in mismatch patients is associated with increased reperfusion/recanalization, but not improved clinical outcomes [Mishra NK et al. Stroke 2010]. This article discusses findings from the Impact of Advanced Neuroimaging on Time to Treatment, Triaging, and Outcomes in Endovascular Stroke Therapy.
- Neuroimaging
- Nursing
A recent meta-analysis reported that delayed thrombosis in mismatch patients is associated with increased reperfusion/recanalization, but not improved clinical outcomes [Mishra NK et al. Stroke 2010]. Dileep R. Yavagal, MD, University of Miami, Miami, Florida, USA, discussed findings from the Impact of Advanced Neuroimaging on Time to Treatment, Triaging, and Outcomes in Endovascular Stroke Therapy.
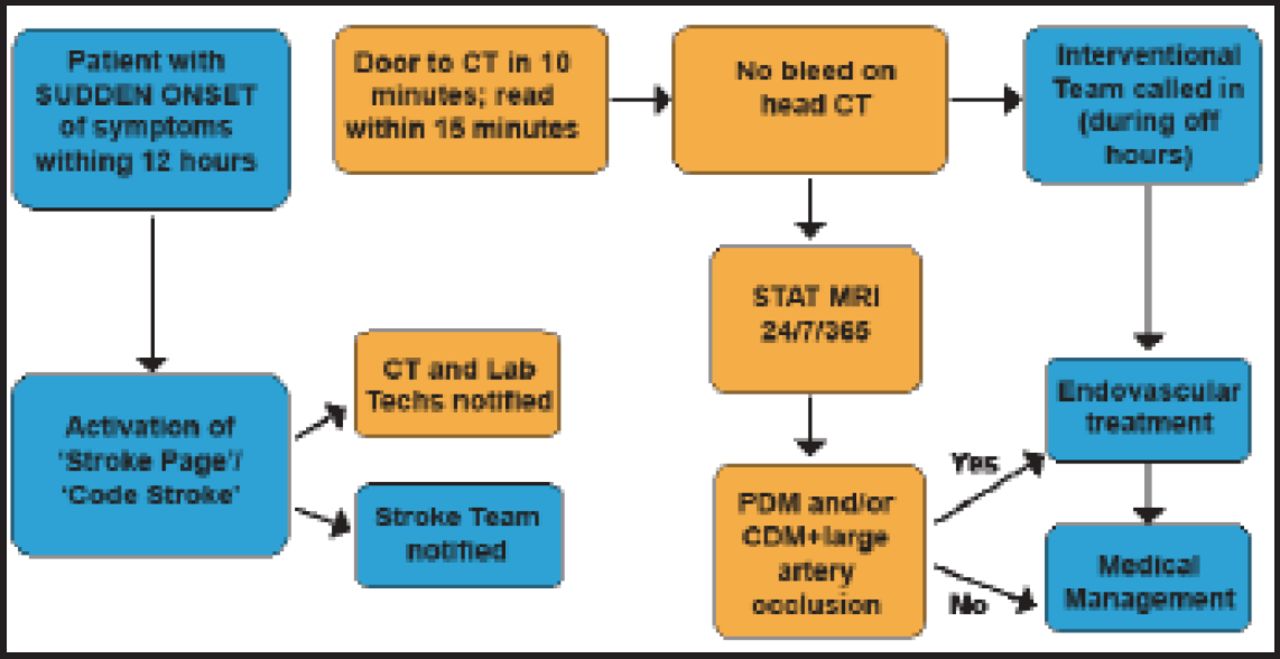
From January 2008 to February 2010, Dr. Yavagal and his associates kept a registry of all consecutive patients undergoing advanced magnetic resonance imaging (MRI) for arterial ischemic stroke (AIS). The objective of the retrospective analysis at their single tertiary care center was to assess the impact of delays associated with the use of advanced neuroimaging on triage and clinical outcomes. Their treatment algorithm (Figure 1) provided computed tomography (CT) for every patient except those with hemorrhage, followed by MRI. Those with a mismatch received endovascular treatment.

MIAMIS Treatment Algorythm.
Reproduced with permission from DR Yavagal, MD.
Inclusion criteria included patients who presented 0 to 12 hours from symptom onset, with an NIHSS >5 and acute stroke syndrome, a negative CT for bleeding, and the presence of perfusion-diffusion mismatch or core measures plus large vessel occlusion.
A total of 89 consecutive patients with suspected AIS took part in the MRI in Acute Management of Ischemic Stroke (MIAMIS) study. Mean participant age was 65.6±14.8 years; 52.8% were male. Mean NIHSS was 15.5 (range, 9 to 20). The average time from symptom onset (TFSO) to door was 214±144 minutes; TFSO to MRI, 318±151 minutes.
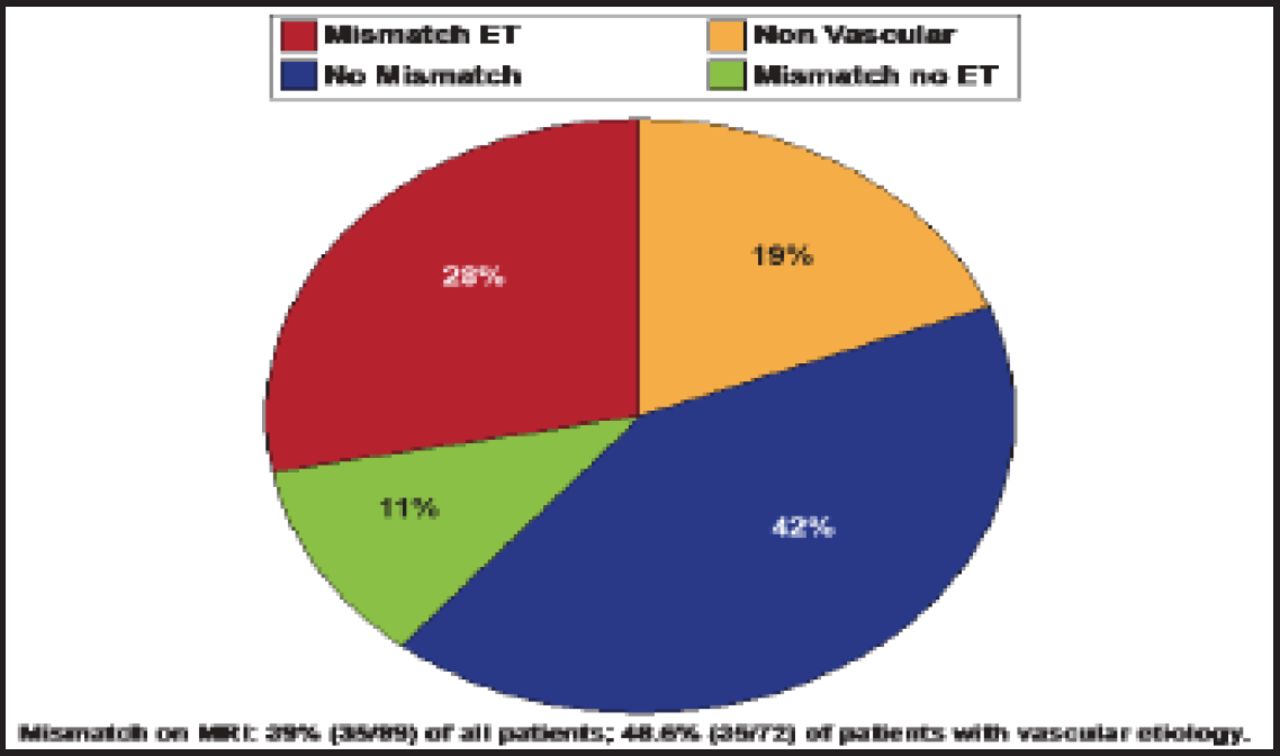
Scans indicated that 39% (35/89) of all patients had a mismatch on MRI. Nineteen percent of all patients had nonvascular etiologies such as seizures or drug overdose (Figure 2). Amongst the patients with vascular etiology, only 48.6% (35/72) of them had mismatch; All told, 28% of patients received endovascular treatment—a small number compared to clinical trials such as EPITETH, with an 86% mismatch rate in 3 to 6 hours, and DEFUSE-I, with 54% in 3 to 6 hours. However, it is important to note that along with the shorter window in these studies, patients with nonvascular etiologies were also not included in the analyses.

MRI Impact on Treatment Triage.
Reproduced with permission from DR Yavagal, MD.
Dr. Yavagal reported a routine turnaround time of ordering MRI to completion of MRI of 100 minutes, with 73 of these minutes attributed to ruling out contraindications and acquiring patient consent and getting the patient on and off the table. Time added is the “Achilles heel” of combined angiography and MRI, he said.
Several trials have tested thrombolysis in patients selected after MRI; some centers have also incorporated mismatch imaging and delayed thrombolysis into their routine clinical practice [Schellinger PD et al. AJNR Am J Neuroradiol 2000]. Two trials, however, claim insufficient evidence to support or refute delayed treatment based on mismatch selection.
Schellinger et al. [Neurology 2010] report that baseline diffusion weighted imaging (DWI) lesion volumes probably predict (final) infarct volumes and possibly predict early and late clinical outcome measures. Baseline perfusion weighted imaging (PWI) volumes predict the baseline stroke severity to a lesser degree compared with DWI. The authors claim insufficient evidence to support or refute the value of PWI in diagnosing acute ischemic stroke.
Mishra et al. [Stroke 2010] examined whether delayed treatment according to the presence of mismatch can be recommended for routine clinical practice. They found that diagnostic criteria are still evolving, and without Phase 3 validation of the mismatch selection paradigm, delayed treatment, even according to mismatch selection, cannot be recommended as part of routine care.
ENACT. Table 1. Clinical Outcomes.
SPS3. Table 1. Major Hemorrhages.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.