

Summary
The use of multimodal imaging is increasing, with the hope that it will improve patient selection for endovascular stroke treatment. This article discusses the effects of time delays on outcomes and hemorrhage rates in patients who receive noncontrast computed tomography only or multimodal CT imaging, as well as the DIFFUSE-2 and Multi MERCI Trials.
- Interventional Techniques & Devices
- Ischemia
- Interventional Techniques & Devices
- Cerebrovascular Disease
The use of multimodal imaging is increasing, with the hope that it will improve patient selection for endovascular stroke treatment. A recent post hoc analysis of the Interventional Management of Stroke I-II trial suggests a 12% decrease in the probability of a good outcome for every 30 minutes of delay from symptom onset to the initiation of endovascular treatment [Khatri P et al. Neurology 2009]. Rishi Gupta, MD, Emory School of Medicine, Atlanta, Georgia, USA, discussed the effects of time delays on outcomes and hemorrhage rates in patients who receive noncontrast computed tomography (NCCT) only or multimodal CT imaging.
Patients with occlusion of the middle cerebral artery (MCA; M1 or M2) or internal carotid artery who were treated <8 hours from symptom onset were in a retrospective review of patients at eight tertiary stroke centers. From September 2009 to December 2011, a total of 594 patients were screened; 418 were included in the study. Data were collected on time points for every milestone, as well as on demographics, radiographic interpretation of hemorrhages, and reperfusion status. Infarct volume was calculated using summation of region of interest of each slice.
Successful reperfusion was defined as Thrombolysis in Cerebral Infarction (TICI) score 2b or better. Asymptomatic hemorrhage was defined as H1, H12, or PH1, based on the European Cooperative Acute Stroke Study (ECASS) definition. Modified Rankin scale score at 90 days was used to assess outcomes from 0 to 2.
Baseline demographics were comparable between the NCCT (n=227) and CT perfusion (n=191) groups, except patients in the NCCT group were noted to have a higher pretreatment NIHSS (19±6 vs 17±6; p<0.01). Patients who were undergoing CT perfusion prior to reperfusion had significantly longer times from CT acquisition to groin puncture (121±68 min vs 81±61 min; p<0.001) and from CT acquisition to reperfusion (223±89 min vs 175±94 min; p<0.001) compared with NCCT. There were no differences in good outcomes or intracranial hemorrhage between the two groups.
Overall, use of multimodal CT imaging led to significant delays in acute endovascular care. Additional imaging did not translate to better clinical outcomes or reduce hemorrhagic rates. These results suggest that the streamlining of treatment will require rapid triage and that NCCT may be sufficient to select patients for endovascular therapy and achieve faster reperfusion.
DEFUSE-2: Target Mismatch and Favorable Clinical Outcomes
The DEFUSE-1 study identified a specific magnetic resonance imaging (MRI) profile (Target Mismatch [TMM]; Table 1) that is associated with benefit from reperfusion in IV tissue plasminogen activator (tPA)-treated patients. It was unknown whether local investigators in the acute setting could accurately determine a patient's TMM status or if patients with that profile would respond more favorably to endovascular reperfusion than those without it.
Definition of TMM.
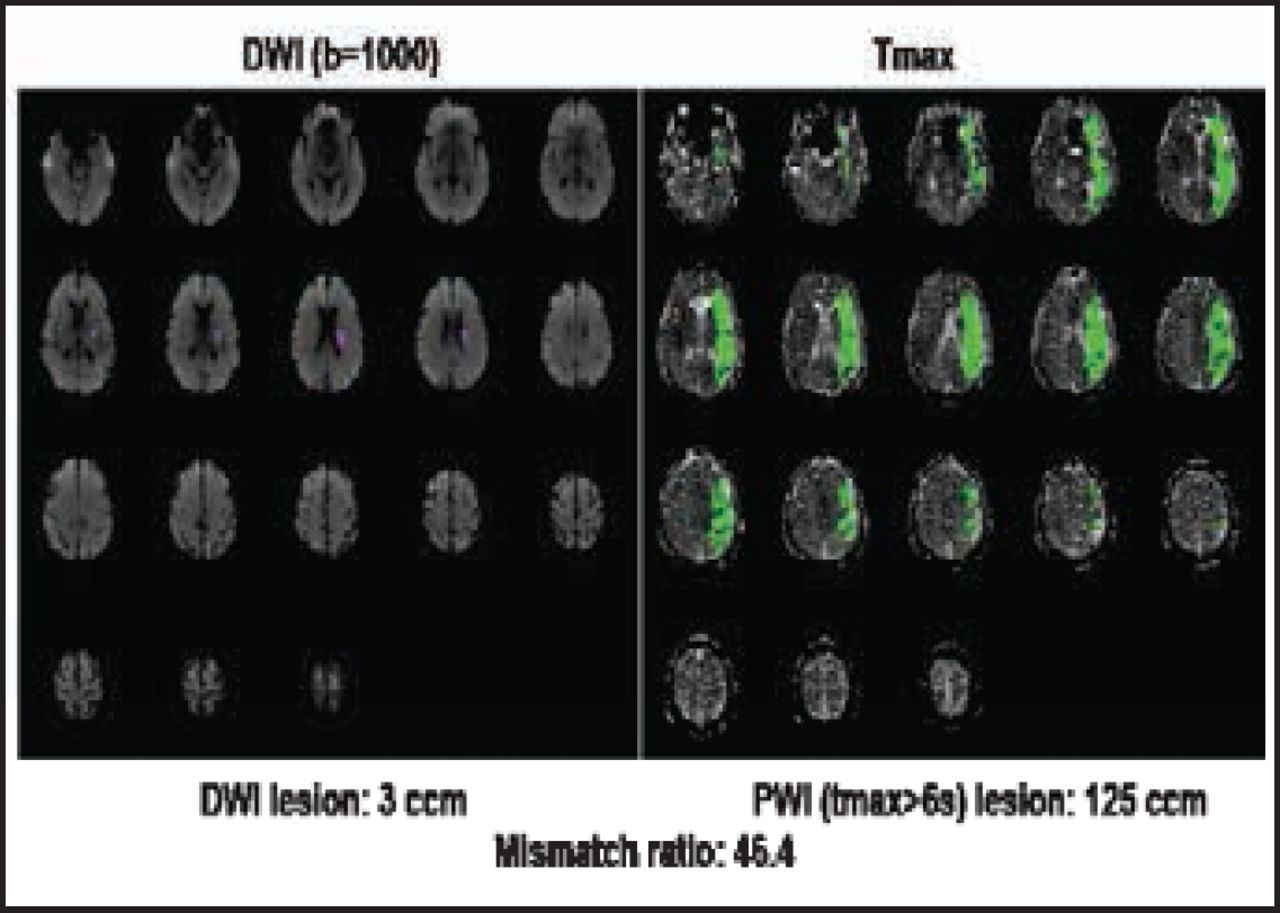
The aim of Diffusion-Weighted Imaging Evaluation for Understanding Stroke Evolution Study-2 [DEFUSE-2; NCT01349946] was to demonstrate that clinicians in the emergency setting, with the aid of RAPID—a fully automated MRI analysis program that outlines and measures perfusion-weighted imaging and diffusion-weighted imaging lesions (Figure 1)—can identify MRI profiles that predict clinical and radiographic outcomes following endovascular reperfusion. Maarten G. Lansberg, MD, PhD, Stanford University, Palo Alto, California, USA, reviewed clinical endpoint results from DEFUSE-2.

RAPID—Automated MRI Analysis Program That Outlines and Measures PWI and DWI Lesions.
Reproduced with permission from MG Lansberg, MD, PhD.
The multicenter, prospective cohort study enrolled 138 patients from 2009 to 2011. Study participants had NIHSS ≥5, were aged ≥18 years, were scheduled to undergo acute stroke therapy (groin puncture <12 hours from symptom onset), and were able to undergo an MRI stroke study <90 minutes prior to the start of the intraarterial procedure. The DEFUSE-2 protocol called for serial MRI imaging before and after endovascular therapy and Day 30 clinical assessment (NIHSS and Rankin).
One hypothesis was that investigators in multiple clinical sites can quickly and accurately establish the MR profile of acute stroke patients using RAPID. In the DEFUSE-2 study, there was 97% agreement between local investigators and the core imaging laboratory in assessment of TMM status. The other hypothesis was that patients with a TMM would respond more favorably to endovascular reperfusion therapy than patients without it.
The primary analysis—a comparison of the odds ratios (OR) for the association between reperfusion and favorable clinical response in TMM (n=78) versus No TMM (n=21) patients—showed a significant association between reperfusion and favorable clinical response in TMM patients (OR, 5.0; 95% CI, 1.9 to 13.0) but not in patients without TMM (OR, 0.2; 95% CI, 0.0 to 1.4). The difference between the two ORs was significant (p=0.004).
The authors concluded that local investigators in the acute stroke setting, with the aid of RAPID software, can accurately identify which patients have the TMM profile. Patients in this group have an increased chance of favorable clinical outcomes with early reperfusion, whereas there was no signal of benefit from reperfusion in the non-TMM group.
Multi MERCI – Upgrading Metrics for Recanalization and Reperfusion
David S. Liebeskind, MD, UCLA Stroke Center, Los Angeles, California, USA, discussed how angiographic definitions for revascularization of arterial occlusion often vary in endovascular stroke trials and how TIMI scores continue to be used despite inconsistent methods and limited correlation with clinical outcome after stroke.
Arterial Occlusive Lesion (AOL) and Thrombolysis in Cerebral Infarction (TICI) metrics of recanalization and reperfusion are better options, but detailed questions persist about scale implementation. To address these issues, Dr. Liebeskind and colleagues conducted a prospective analysis of central core lab angiography scores with local site reads in Multi MERCI [NCT00318071]. Their objective was to establish AOL and TICI metrics of recanalization and reperfusion, linking revascularization and clinical outcomes.
Data showed that local-site TIMI score had a modest but statistically significant correlation with AOL recanalization (p<0.001) and TICI reperfusion (p<0.001). Interrater reliabilities of central readers were excellent for AOL (k=0.987) and TICI (k=0.826); AOL and TICI were moderately correlated (p<0.001). AOL recanalization was associated with time from symptom onset to procedure (p=0.005), platelet count (p=0.043), and systolic blood pressure <150 mm Hg (p=0.022). TICI reperfusion was associated with time from symptom onset to procedure (p=0.029), current smoking (p=0.042), congestive heart failure (p=0.031), and systolic blood pressure <150 mm Hg (p=0.013).
Across all grades, TICI reperfusion was inversely associated with 90-day death (p=0.007) and positively associated with good outcomes (p=0.003). AOL recanalization showed the same trend, although the association was weakened (p=0.129; p=0.047).
The optimal TICI score was 2b/3. It strongly predicted 90-day modified Rankin scale 0–2 (OR, 2.73; p=0.004) and decreased mortality (OR, 0.29; p<0.001) beyond AOL 2/3 (OR, 2.78; p=0.020; OR, 0.56; p=0.125). AOL and TICI exhibited similar relationships across various sites of arterial occlusion.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.