

Summary
Noninvasive techniques for cardiac imaging have the potential to offer patients diagnostic assessment with less risk and lower cost than invasive methods; however, currently available modalities focus on anatomical assessment of the heart—not physiology. Cardiac imaging continues to advance, and research is confirming an important role for such modalities as coronary computed tomography angiography, coronary artery calcium testing, and 4-dimensional flow magnetic resonance imaging.
- Cardiac Imaging Techniques
- Emergency Radiology
- Imaging Modalities
Noninvasive techniques for cardiac imaging have the potential to offer patients diagnostic assessment with less risk and lower cost than invasive methods; however, currently available modalities focus on anatomical assessment of the heart—not physiology. Cardiac imaging continues to advance, and research is confirming an important role for such modalities as coronary computed tomography angiography (CCTA), coronary artery calcium (CAC) testing, and 4–dimensional flow magnetic resonance imaging (4D flow MRI). Research is also helping to define the specific patient populations and situations for which these techniques are most appropriate.
CCTA in the Emergency Department (ED)
The diagnosis of acute coronary syndrome (ACS) in the ED is challenging. Clinical measures, such as history, electrocardiogram (ECG), biomarkers, and clinical scores, are helpful if the findings are clearly positive, but many patients fall into an intermediate– or low–risk group. This is particularly the case for the group of patients who present with typical ischemic symptoms but negative cardiac biomarkers (eg, unstable angina [UA]). Although this population is shrinking as a result of increasingly sensitive biomarker assays, additional tests to help exclude acute coronary disease in these patients are needed. “We need to define the pathway with the strongest negative predictive value—those are the patients who can go home from the emergency room,” said Ronald P. Karlsberg MD, FACC, FSCCT, Cedars Sinai Heart Institute and the Cardiovascular Research Foundation of Southern California, Beverly Hills, California, USA.
The sensitivity and specificity of CCTA (95% and 83%, respectively) are better than or similar to those of exercise ECG, echocardiography, and nuclear testing. More importantly, a very high negative predictability is the strongest feature of CCTA, with a negative predictive value of 99% to 100% in more than 20 studies. Strong negative predictability is the driving characteristic that makes the potential use of CCTA in the ED compelling.
Many patients who are evaluated for ACS in the ED have nondiagnostic ECG findings and normal biomarker levels. CCTA is appropriate for this subset of low– to intermediate–risk patients that would benefit from imaging, said Dr. Karlsberg. He noted several trials that were presented at the 2012 American College of Cardiology (ACC) meeting on the value of CCTA in the ED, in particular the prospective, randomized, multicenter trials ACRIN PA 4005 [Litt HI et al. N Engl J Med 2012; see p. 12 of this report] and ROMICAT II [NCT01084239; see p. 20 of this report]. These trials all show uniform findings of reduced time to diagnosis, early ED discharge, increased efficiency in the ED, reduced ED cost, more precise definition of patients with disease, lower radiation exposure compared with exercise nuclear testing, and low event rates out to 2 years, with the opportunity to reduce repeat visits to the ED visits. One of the largest real–world efforts is being carried out at Miami Baptist Hospital; the use of CCTA in the ED has led to 85% of patients being discharged home (including those with no or mild nonobstructive disease), a 50% reduction in the length of stay, a decrease in cost of $1000 per patient, and a rate of major adverse cardiovascular (CV) events of 0.1% at 30 days [Registry for Cardiac Perfusion CT; NCT 01346605].
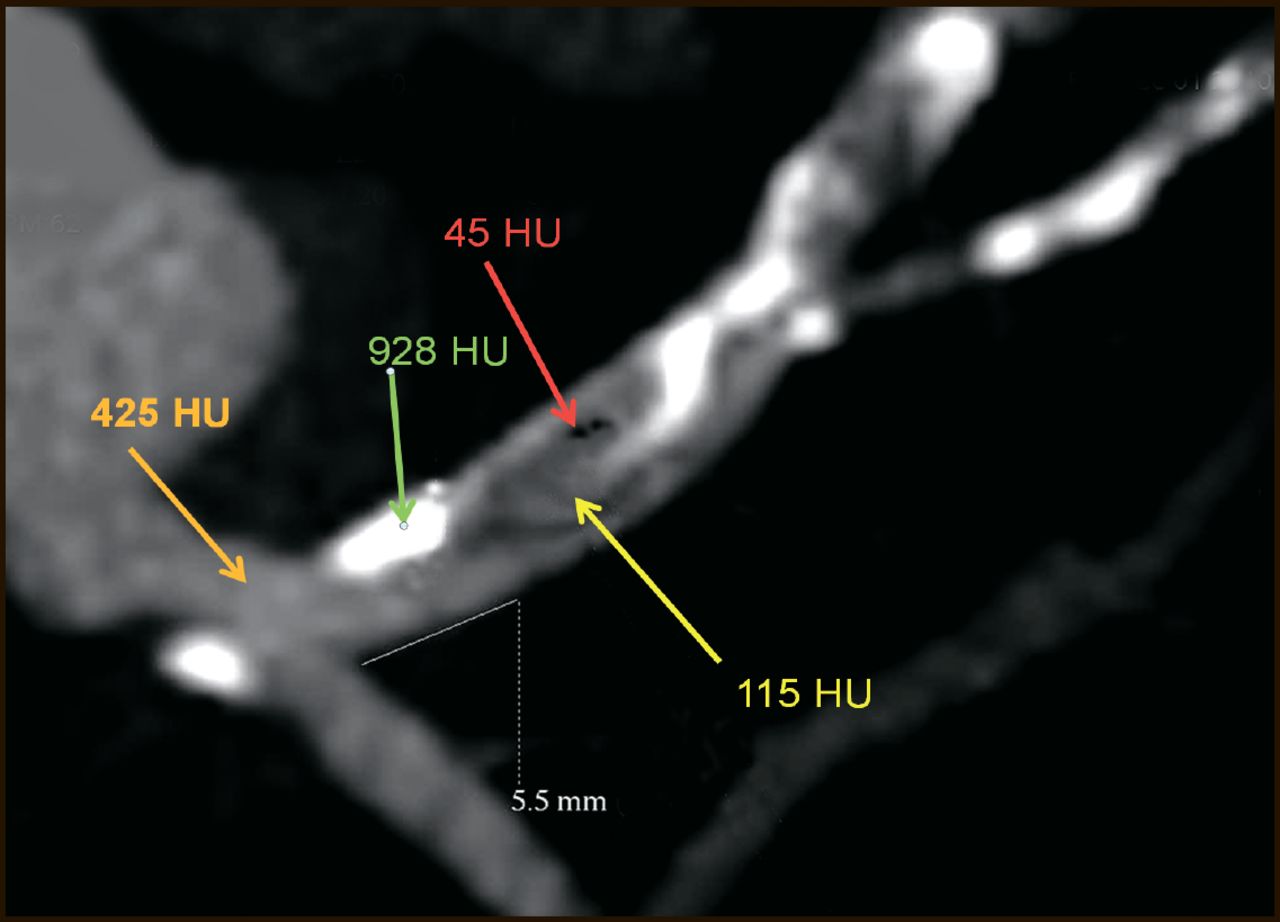
According to a 2011 focused update of the ACC/American Heart Association (AHA) guidelines for UA/non–ST–elevation myocardial infarction, CCTA now has a class IIa–B recommendation in the initial assessment of patients with chest pain who are at low to intermediate risk [Anderson JL et al. Circulation 2011]. Numerous other organizations, including the European Society of Cardiology, the Society of Cardiovascular Computed Tomography, and the American College of Radiology, have endorsed the use of CCTA to determine the extent of coronary artery disease (CAD) or the culprit lesion in ACS. Also, government and private health insurance programs are paying for the use of CCTA in the ED. Further, current studies have demonstrated that noncalcified plaque with characteristics of vulnerability is a potentially important prognostic finding that predicts future ACS and myocardial infarction (MI). CCTA can help stage and time intervention (Figure 1). Although these data are very encouraging, it is important to acknowledge that not all studies have shown reductions in total cost with CCTA, and none has shown improved clinical outcomes with this modality compared with standard care.

CCTA from a 70–Year–Old Man with Chest Pain, Modest Risk Factors, and No Known Previous CAD.
CCTA was performed, and hours later, a minimal troponin leak was determined. CCTA defined the Hounsfield Units (HU) characteristic of the contrast agent 425 HU, dense calcified plaque 928 HU, noncalcified plaque 115 HU, and low–density (potentially vulnerable) plaque 45 HU. Positive remodeling, another characteristic of vulnerability, was present. The culprit narrowing was 5.5 mm from the left main, providing an invasive coronary angiography strategy for subsequent successful stenting of the proximal left anterior descending coronary artery, which was expediently performed (Cedars Sinai Medical Center, Los Angeles California). With permission from RP Karlsberg, MD.
To date, CCTA has not been used widely in the ED, although the results of recent larger–scale randomized studies and updated recommendations are likely to lead to expanded use. When implementing CCTA in an emergency setting, it is critical that appropriate equipment, training, and expertise be in place to achieve results that are similar to those in the presented published studies. Patients need to be prepared for the test with medication to lower the heart rate, preferably <60 beats per minute, which ensures high quality images and low radiation exposure. Importantly, this preparation is not possible in all patients, and those with insufficient heart rate control cannnot be adequately evaluated with this modality. Also, not all patients will benefit from CCTA, Dr. Karlsberg emphasized. CCTA is not appropriate for patients with high–risk ACS, known obstructive disease, renal impairment, an uncontrolled heart rate after beta–blockers or arrhythmias, an allergy to contrast medium, or severe coronary calcium or when patients are not cooperative and can not hold their breath. Furthermore, there are some patients in whom, based on clinical judgment, absolutely no further testing is required. An optimal pathway has not been established yet, but a large group of low–to–intermediate risk patients may substantially benefit from this new approach. Consequently, this recently released research paves the way for appropriate and more widely adopted implementation of CCTA in the ED for rapid evaluation of chest pain.
Prognostic Value of CCTA
In addition to its high negative predictive value, CCTA has high sensitivity, said Benjamin Chow, MD, FRCPC, FACC, FASNC, FSCCT, Co–Director of Cardiac Radiology and Director of Cardiovascular CT, University of Ottawa Heart Institute, Ottawa, Ontario, Canada. A recent meta–analysis found an average sensitivity of 98% across several single–center studies [Paech DC et al. BMC Cardiovasc Disord 2011]. The first results from multicenter trials showed variable operating characteristics, with a lower mean sensitivity (90%). Dr. Chow pointed out that one study showed that sensitivity and negative predictive value vary widely according to center and that this highlights the need for individual centers to perform validation testing.
More recent multicenter studies have demonstrated the independent and incremental value of CCTA in predicting all–cause mortality among symptomatic patients with CAD [Min JK et al. JACC 2007; Ostrom MP et al. JACC 2008]. Increasing severity of disease on CCTA has consistently been associated with worse outcomes, and the risk for death is extremely low for patients with no evidence of CAD on CCTA. In his own study, Dr. Chow and colleagues analyzed data from an international multicenter registry (CONFIRM) in 27,125 patients and found that CCTA conveys prognostic information above left ventricular ejection fraction [Chow BJ et al. Circ Cardiovasc Imaging 2011]. The annual mortality for patients with no evidence of CAD on CCTA was 0.65%, compared with an annualized mortality rate of 1.14% for patients with nonobstructive CAD and 2.63% for patients with high–risk CAD. These data confirm the results of prior studies that have shown a similar association between burden of CAD and outcomes using other imaging modalities (eg, coronary angiography, nuclear imaging).
Coronary Artery Calcium (CAC)
In light of the value of CCTA, is there still a role for CAC testing? Although CCTA is the noninvasive test of choice in many cases, the test is more expensive and time–intensive, requires greater skill for interpretation, and uses higher doses of radiation, according to Khurram Nasir, MD, MPH, Yale University School of Medicine, New Haven, Connecticut, USA. Dr. Nasir said that CAC testing has a role in testing asymptomatic and symptomatic patients with varying levels of risk and is of little value for people who are at very high risk for CAD.
An important feature of CAC is that the absence of CAC indicates a very low risk for CAD. Large studies have shown that the rate of CV disease events or death at 4 to 5 years is less than 1% for patients with a CAC score of 0 [Sarwar A et al. JACC Imaging 2009; Budoff M et al. Am Heart J 2009]. The results of a 2011 study that involved the CONFIRM registry showed that among patients with a CAC score of 0, 84% had no CAD, 13% had nonobstructive CAD, and 3.5% had ≥50% stenosis [Villines TC et al. JACC 2011]. With negative predictive values of 96% and 98% for stenosis of ≥50% and ≥70%, respectively, CAC testing can reliably exclude coronary disease, said Dr. Nasir.
Studies have demonstrated that neither CCTA nor CAC scoring offers added benefit over the other among asymptomatic patients [Hadamitzky M et al. Circ Cadiovasc Imaging 2011; Kwon SW et al. Radiology 2011]. “Even if CCTA could detect and prevent events, the number needed to scan in the absence of a CAC of 0 is staggeringly high,” said Dr. Nasir. To identify “potential misses” with a CAC score of 0, 338 scans would be needed to prevent 1 late revascularization, 947 would be needed to prevent 1 myocardial infarction, and 1597 would be needed to prevent 1 death. Guidelines that were issued by the European–based National Institute for Health and Clinical Excellence recommend no further testing for people who have a CAC score of 0.
According to an ACC/AHA clinical expert consensus document, CAC testing can help rule out obstructive CAD in patients who are at low risk of CAD and is a rapid and efficient screening tool for patients in the ED with chest pain and nonspecific ECG findings [Greenland P et al. JACC 2007]. The test also is reasonable for assessing CV risk in asymptomatic adults who are at intermediate risk (10% to 20% 10–year risk) and may be reasonable for people who are at low to intermediate risk (6% to 10%); CAC testing offers no benefit to persons who are at low risk [Greenland P et al. JACC 2010].
4D Flow MRI
The strength of 4 dimensional (4D) flow MRI is its ability to help one gain an understanding of complex situations, said Michael Markl, PhD, Departments of Radiology & Biomedical Engineering, Northwestern University, Chicago, Illinois, USA.
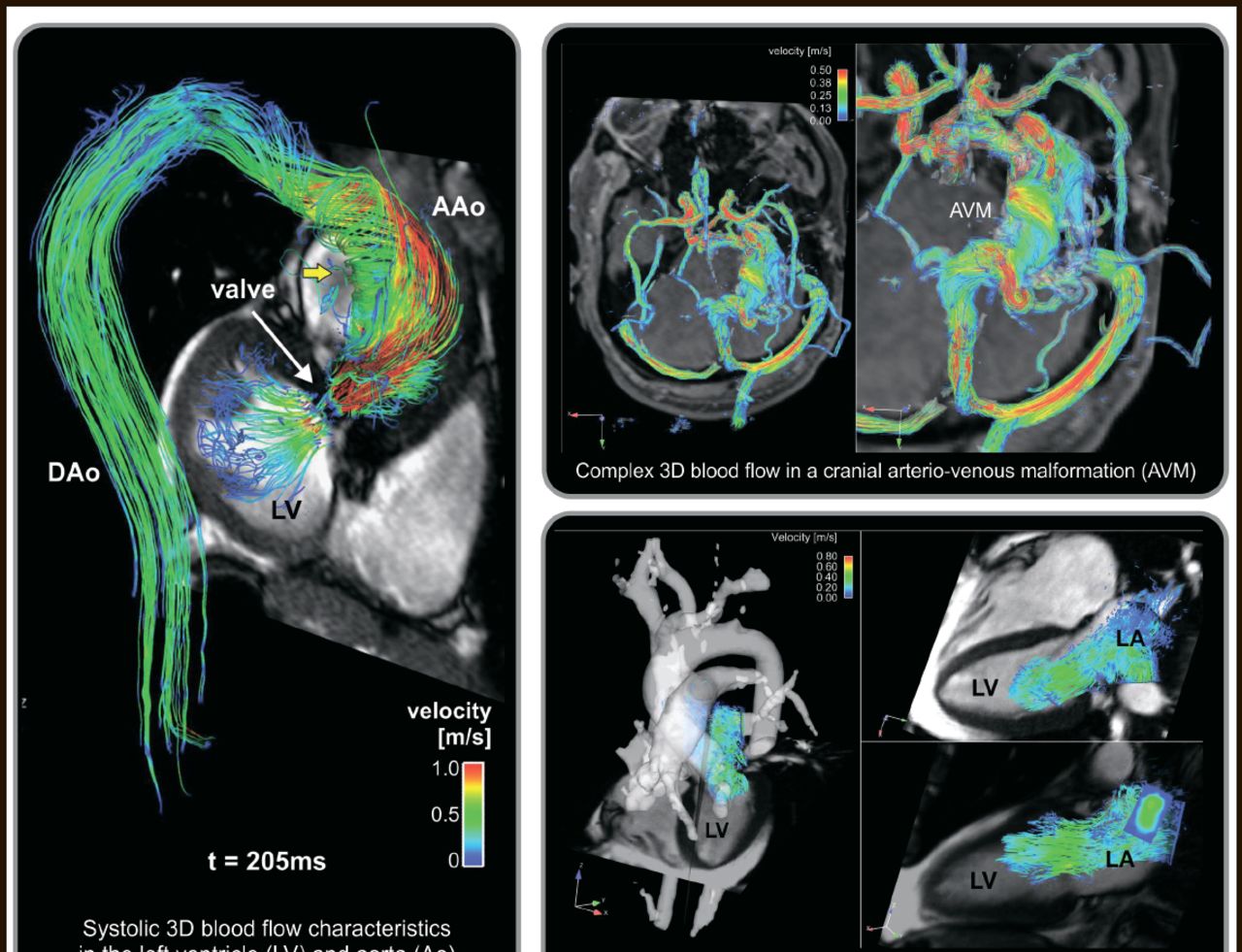
MRI techniques provide noninvasive methods for the highly accurate anatomical depiction of the heart and vessels. The intrinsic motion sensitivity of MRI can be used to image vessels as in phase contrast MR–angiography or to quantify blood flow and motion of tissue. ECG–synchronized flow–sensitive 3D MRI using 3–directional velocity encoding (also termed ‘4D flow MRI’) can be employed to help visualize true 3D blood flow and detect deranged flow patterns with full anatomical coverage of the CV system (Figure 2). Moreover, since 4D flow MRI data reflect the true underlying time–resolved blood flow velocity vector field, it is possible to retrospectively quantify flow rates or derived parameters, such as pressure difference maps and wall sheer stress. Dr. Markl noted that 4D MRI can help quantitate systolic or valve function and discussed various applications. For example, when used in patients with a bicuspid aortic valve, 4D flow MRI showed that flow jet patterns were influenced by the particular morphology of the cusp fusion and that the wall shear stress was significantly different and elevated between patients with an aortic aneurysm and normal tricuspid valves and those with a bicuspid aortic valve with fused right and left leaflets.

4D Flow MRI.
Reproduced with permission from M. Markl, PhD.
4D flow MRI can also be used as a complement to CCTA and standard MRI to evaluate the results of transcatheter aortic valve implantation. Initial results suggest that aortic root reconstruction may produce a favorable postinterventional hemodynamic outcome, said Dr. Markl, “but flow was shown to still be substantially deranged, increasing the risk for postoperative aortic aneurysm and dilation.”
The technique can also be used to look at the entire heart and surrounding vascular structure, as in evaluating the complex hemodynamic situation in patients with congenital heart disease, such as switch repair for the transposition of the great arteries. Several groups have reported advances in the application of 4D flow MRI to other vascular regions, including peripheral vessels, carotid arteries, and large intracranial arteries and the pulmonary and venous systems.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.