

Summary
For most clinicians, one of the most anticipated guideline updates is the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8). The JNC 8 has been in development for some time and is expected to be released by the end of 2012. This article provids an update on the process and timing for these eagerly awaited guidelines.
- Cardiology Guidelines
- Hypertensive Disease
For most clinicians, one of the most anticipated guideline updates is the Eighth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 8). The JNC 8 has been in development for some time and is expected to be released by the end of 2012. Suzanne Oparil, MD, University of Alabama, Birmingham, Alabama, USA, provided an update on the process and timing for these eagerly awaited guidelines.
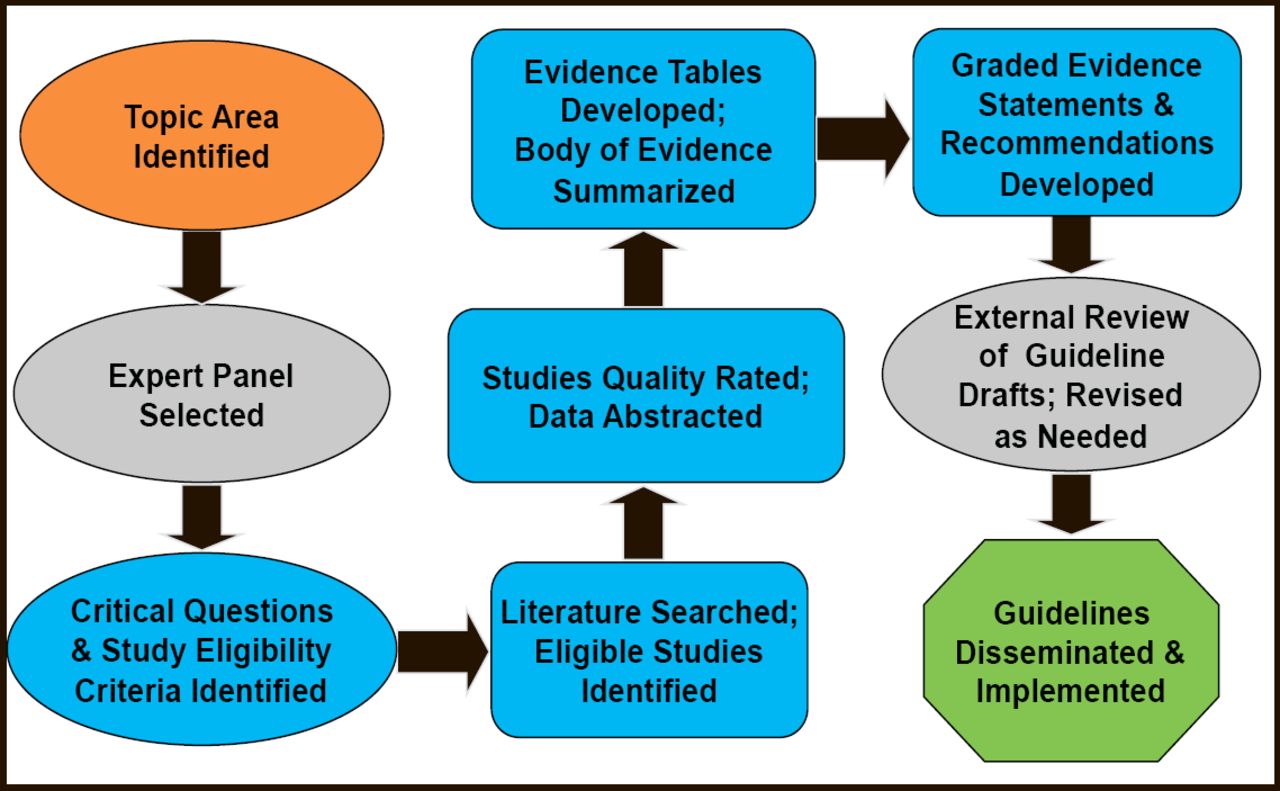
A fundamental change, and part of the reason for the delay in issuing the guidelines, noted Dr. Oparil, is the adoption of a rigorous nine–step systematic review and development process (Figure 1). Previous versions of the guidelines have received criticism for relying too heavily on low–level evidence and consensus [Tricoci P et al. JAMA 2009], and this new, more rigorous approach will result in guidelines that are strictly evidence–based. The recommendations will draw from the results of randomized controlled trials (RCTs) that assess important health outcomes rather than intermediate or surrogate endpoints. The new approach also involves an expanded group of experts on the guideline committee, which now includes expertise in hypertension, primary care, cardiology, nephrology, clinical trials, research methodology, evidence–based medicine, epidemiology, guideline development and implementation, nutrition/lifestyle, nursing, pharmacology, systems of care, and informatics. Senior scientists from the National Heart, Lung, and Blood Institute (NHBLI) and National Institute of Diabetes and Digestive and Kidney Diseases have also joined the panel as nonvoting members.

NHBLI Systematic Review and Guideline Development Process.
Reproduced with permission from S. Oparil, MD.
The JNC 8 is expected to focus on three major areas: the threshold blood pressure (BP) for drug therapy initiation, the target BP for drug therapy, and the most appropriate drugs to achieve the target BP. Prespecified subgroups of interest include patients with diabetes, chronic kidney disease (CKD), coronary artery disease, peripheral artery disease, or heart failure (HF); older patients; men and women; and racial and ethnic groups. Outcomes will focus on overall, cardiovascular (CV), and CKD mortality, myocardial infarction, HF, hospitalization for HF and stroke, coronary and peripheral revascularization, and end–stage renal disease.
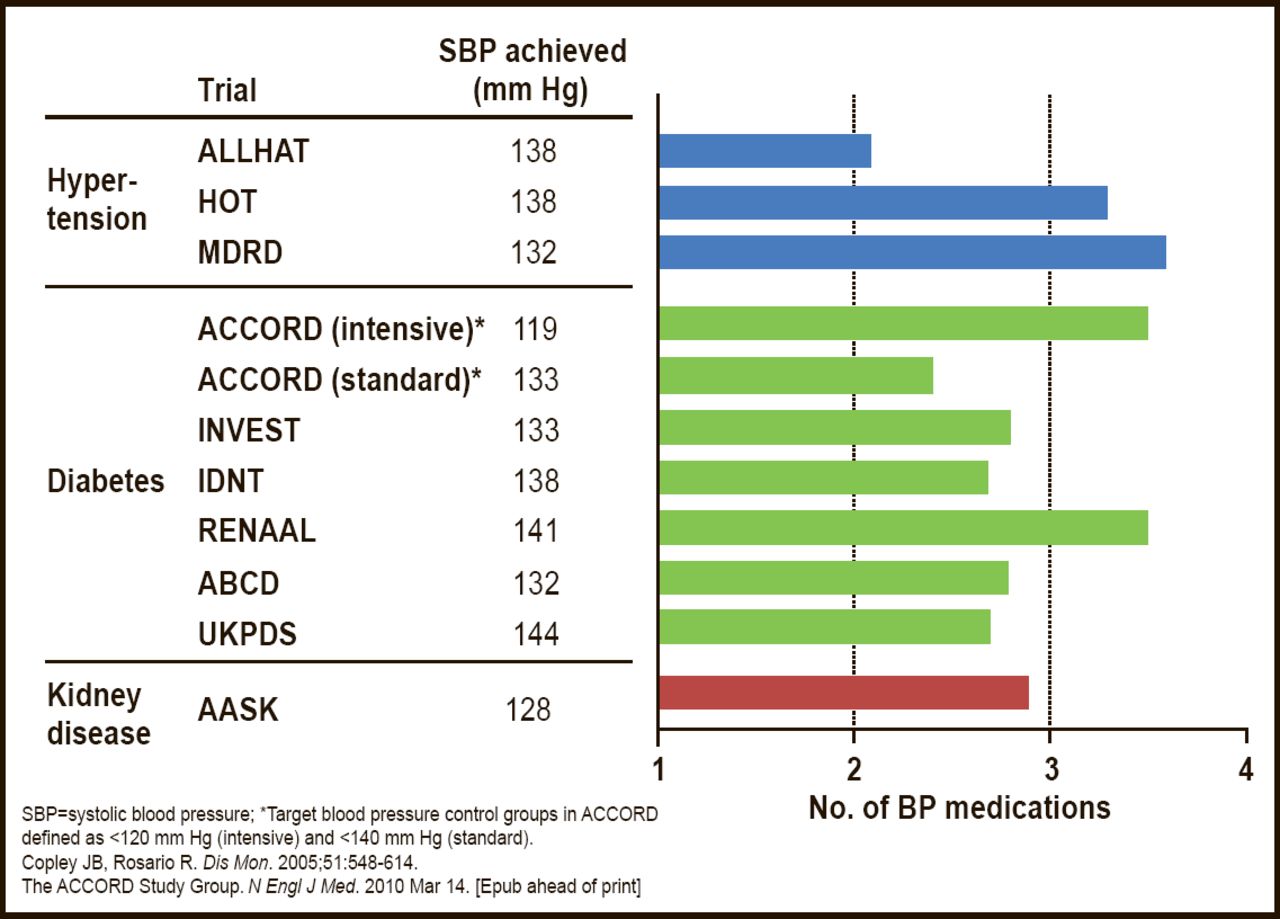
Using the JNC 7 as a backdrop, Kenneth A. Jamerson, MD, University of Michigan, Ann Arbor, Michigan, USA, discussed the initial choice of therapy for hypertensive patients who are at low and high risk for CV events. In general, Dr. Jamerson stressed the importance of combination therapy, noting that nearly all monotherapy trials for BP control were “in essence combination therapy trials anyway” (Figure 2). As an example of risk–stratified recommendations, he reviewed the 2010 Updated Consensus on the Management of Blood Pressure in Blacks, issued by the International Society for Hypertension in Blacks [Flack JM et al. Hypertension 2010]. For primary prevention in low–risk patients with BP ≥135/85 mm Hg but without target–organ damage or overt or preclinical cardiovascular disease (CVD), this consensus document recommends a modest lowering of target BP to <135/85 mm Hg using lifestyle modification and drug therapy. For patients in this group whose BP is consistently <145/90 mm Hg, the recommendations encourage the use of comprehensive lifestyle modification for up to 3 months without concurrent drug therapy. For high–risk patients with BP ≥130/80 mm Hg and target–organ damage, preclinical CVD, or the presence or history of CVD, these consensus guidelines recommend a lower BP target of <130/80 mm Hg using both lifestyle modification and drug therapy. As to the choice of drug therapy, Dr. Jamerson sees no advantage to using diuretics as initial therapy, suggesting that both high– and low–risk patients benefit more from combination therapy (preferably with an ACE inhibitor and amlodipine), as it provides prompt and efficient BP control. Given the importance and proven efficacy of lifestyle modification in reducing BP, Dr. Jamerson suggested an article by Scisney–Matlock M. et al. in Postgrad Med 2009 as a good resource for those who are interested in strategies to overcome the barriers to patient compliance.

Multiple Medications Are Required to Achieve BP Control in Clinical Trials.
Reproduced with permission from WC Cushman, MD.
Current target BP guidelines are not drawn from RCTs; rather, they are based on a general acceptance of the concept that “lower is better,” particularly so for patients who are at higher risk. One of the major unknowns with the JNC 8 is whether there will be changes to BP targets. William C. Cushman, MD, Veterans Affairs Medical Center and University of Tennessee College of Medicine, Memphis, Tennessee, USA, discussed why he believes that there are good reasons for the guidelines not to go below BPs that have been proven in RCTs, although he emphasized that this was his opinion and not to be assumed what JNC 8 will recommend. These include:
-
A much larger proportion of the population of the United States will be classified as having hypertension that presumably needs drug therapy [Greenlund KJ et al. Arch Intern Med 2004]
-
Patients who were previously classified as having hypertension will require more drugs to achieve lower BP goals [Cushman WC et al. N Engl J Med 2010]
-
Treating to lower BP targets at a population level may be harmful, in that some patients may achieve BP levels that are too low (a concept known as the J–curve) [Messerli FH et. al. Ann Intern Med 2006]
-
If neither beneficial nor harmful, resources would be wasted and, importantly, patient adherence may suffer
“If we are to use RCTs to set BP targets, what is the evidence?” asked Dr. Cushman. For diastolic targets, he noted that several trials have demonstrated a consistent reduction in CV events using a diastolic goal <90 mm Hg. Examples includes the landmark VA Cooperative Morbidity Trial in Hypertension [Veterans Administration Cooperative Study Group on Antihypertensive Agents. JAMA 1967 and 1970] and the Hypertension Detection and Follow–up Program [HDFP Cooperative Group. JAMA 1979]. At least one trial, the Hypertension Optimal Treatment (HOT) study [Hansson L et al. Lancet 1998], did ask the question “Is lower better?” for diastolic BP, noted Dr. Cushman, and the results showed that for most patients, there is neither benefit nor harm with going below a diastolic BP of 90 mm Hg. As for systolic targets, there is good RCT evidence for a systolic BP target of <150 mm Hg (Table 1), but there is no strong support from RCTs for a target of 140 mm Hg or lower (Table 2).
Systolic BP trials Testing SBP Goals and Showing CVD Benefit.1
Trials Testing Systolic BP Goal <140 mm Hg.
RCT data support BP goals of <150/90 mm Hg in most hypertensive patients; however, a goal of <140/90 mm Hg may still be reasonable, especially for patients aged under 60 years or with CKD. In hypertensive patients with diabetes, RCTs support BP goals of 140–150/80–85 mm Hg or lower. The ACCORD BP Trial did not prove CVD benefit for a systolic goal <120 mm Hg compared with a goal of <140 mm Hg [Cushman WC et al. N Engl J Med 2010]. SPRINT and several other trials are testing lower BP goals that may provide more clarity regarding optimal BP targets. Regardless of the results, these important studies of lower BP targets will need to be incorporated into future guidelines.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.