

Summary
Treating to target is the mainstay of EULAR recommendations for the management of patients with rheumatoid arthritis (RA), but is it associated with meaningful clinical outcomes? Eight-year results from the Clinical and Radiographic Outcomes of Four Different Treatment Strategies in Patients with Early Rheumatoid Arthritis study [BeST] suggest that the answer is yes.
- Rheumatoid Arthritis Clinical Trials
- Featured Meeting - Specialty page
Treating to target is the mainstay of EULAR recommendations for the management of patients with rheumatoid arthritis (RA), but is it associated with meaningful clinical outcomes? Eight-year results from the Clinical and Radiographic Outcomes of Four Different Treatment Strategies in Patients with Early Rheumatoid Arthritis study [BeST] suggest that the answer is yes. Marianne van den Broek, MD, Leiden University Medical Center, Leiden, The Netherlands, reported that after 8 years of targeted treatment, radiological damage was still very low, and functional ability had been maintained in all groups. Remission percentages were stable at about 52%, and drug-free remission was achieved in 15% to 19% of subjects.
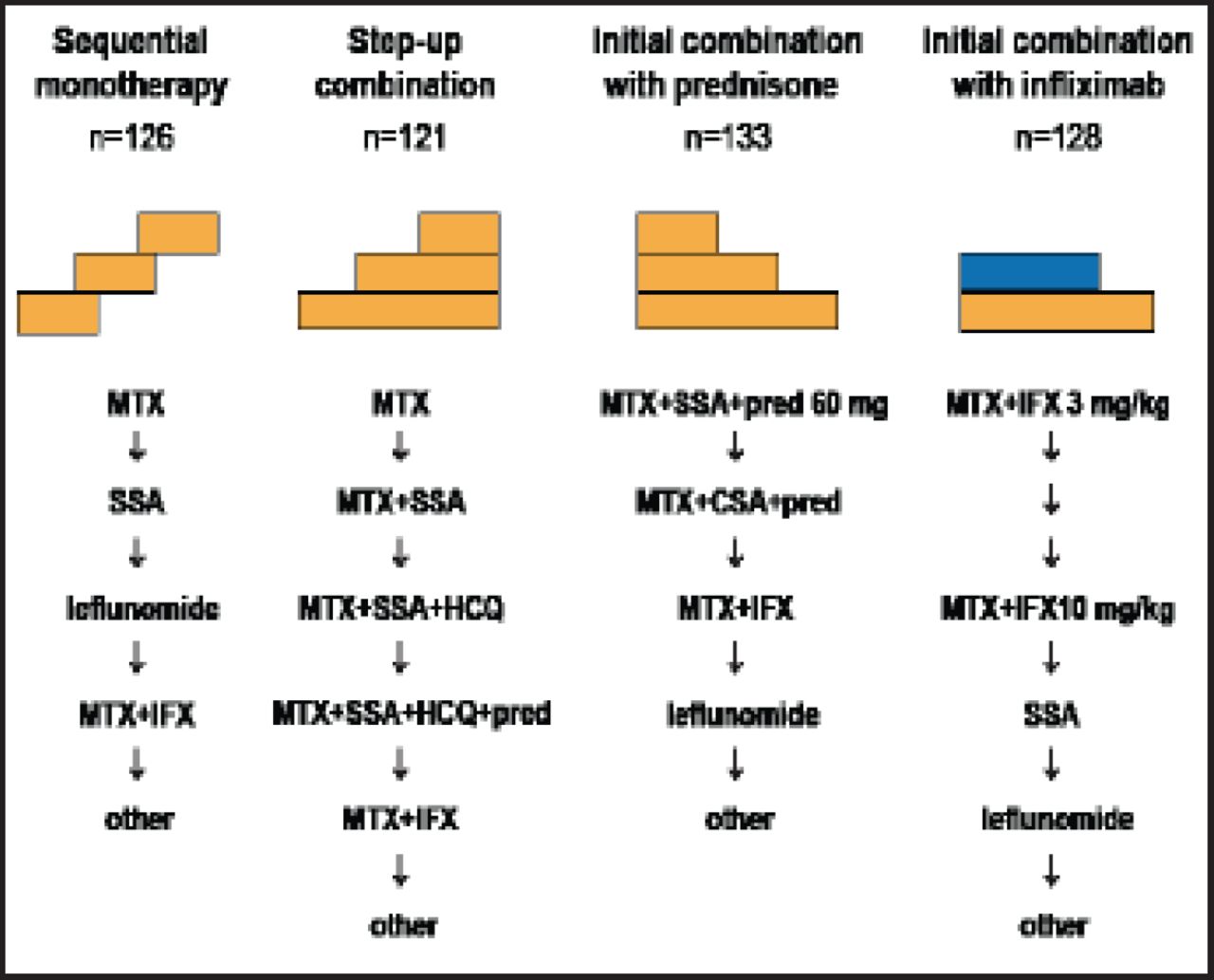
The objectives of the BeSt trial were to compare clinical and radiological outcomes after 8 years of targeted treatment with 4 treatment strategies in patients with recent onset RA. The study comprised 508 patients who had a mean age of 54 years; were mostly women; and had a mean DAS44 of 4.4, mean Health Assessment Questionnaire (HAQ) score of 1.4, and median Sharp-van der Heijde score (SHS) of 4. About two-thirds of the subjects were rheumatoid factor-positive; 62% were anticitrullinated protein antibody-positive. Participants were randomized to 1 of 4 treatment strategies: 1) sequential monotherapy, 2) step-up combination therapy, 3) initial combination with prednisone, and 4) initial combination with infliximab (Figure 1). The treatment target was DAS ≤2.4. Treatment was adjusted every 3 months, based on individual DAS using the following algorithm:
-
DAS >2.4: proceed to the next step in the treatment
-
DAS ≤2.4 for at least 6 months: taper to maintenance dose
-
DAS <1.6 for at least 6 months: stop antirheumatic treatment

Treatment Strategies.
MTX=methotrexate; IFX=infliximab; HCQ=hydroxychloroquine; CSA=cyclosporine; SSA=sulfasalazine.
Reproduced with permission from M. van den Broek, MD.
Functional ability, measured with the HAQ, was analyzed with a linear mixed model, with time, treatment, and time*treatment as independent variables. Radiographs of baseline and Years 1 through 8 were scored with the SHS, blinded for the patient's identity and in random order, to assess radiological damage progression.
After 8 years, 347 (68.3%) patients were still in follow-up. A DAS ≤2.4 was achieved in 79% of these subjects, and 52% were in remission (DAS <1.6). The differences between the treatment groups were not significant (Table 1). Among those who achieved remission, 18%, 19%, 17%, and 15% of the patients in Groups 1 through 4, respectively, were in drug-free remission, with a median (mean) duration of 45 (39) months. Six patients were lost to follow-up, and 12 patients achieved drug-free remission in Year 8, while 8 patients with prolonged drug-free remission dropped out of the study.
Eight-Year Results.
After initial differences in Years 1 and 2 between the 4 groups, annual radiological damage progression rates were low and similar between all groups, reflecting the efficacy of DAS-steered therapy. Median (mean) total damage progression after 8 years was 3 (11) points SHS (nonsignificant between groups). Patients who were in sustained drug-free remission had a mean SHS progression of 0.1 [median (IQR) 0 (0–0.03)] per person-year drug-free.
The initial improvement of function, which occurred earlier in Groups 3 and 4 than in Groups 1 and 2, was maintained without deterioration over 8 years in all groups. No differences were found for functional ability over time, with the exception of better functional ability in Group 4 compared with Group 2 (mean HAQ 0.57 and 0.71, respectively). Toxicity was comparable between the groups (Table 2).
Toxicity Over Eight Years.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.