

Summary
Systemic inflammation in patients with rheumatoid arthritis (RA) leads to a greater risk of cardiovascular (CV) events that are linked to tumor necrosis factor (TNF)-related atherogenesis. Anti-TNF therapies have been shown in observational studies to reduce the risk of CV events in patients with RA. The objective of this retrospective medical record review was to compare the effect of exposure to anti-TNF treatment on the risk of CV events in patients with RA with those who were treated with methotrexate and other disease-modifying therapies.
- Heart Failure Clinical Trials
- Myocardial Infarction
- Rheumatoid Arthritis
Systemic inflammation in patients with rheumatoid arthritis (RA) leads to a greater risk of cardiovascular (CV) events that are linked to tumor necrosis factor (TNF)-related atherogenesis. Anti-TNF therapies have been shown in observational studies to reduce the risk of CV events in patients with RA. The objective of this retrospective medical record review, presented by Michael T. Nurmohamed, MD, PhD, VU University Medical Center and Jan van Breemen Research Institute, Amsterdam, The Netherlands, was to compare the effect of exposure to anti-TNF treatment on the risk of CV events in patients with RA with those who were treated with methotrexate and other disease-modifying therapies.
The study population was drawn from the Thomson Reuters Market Scan Commercial Claims Database between January 1, 2003 and December 31, 2010. Selected patients were required to have at least 2 RA diagnoses and be aged ≥18 years. Patients' records were evaluated from the index date (first anti-TNF prescription fill date or random date for patients without anti-TNF prescription) to the end of health plan enrollment, end of data availability, or 6 months after discontinuation of therapy. The primary endpoint was the composite of myocardial infarction (MI), stroke, unstable angina, or congestive heart failure (CHF). The secondary endpoint was individual CV events. Cumulative exposures were calculated for anti-TNF therapy, methotrexate, other nonbiologic disease-modifying antirheumatic drugs (DMARDs), and corticosteroids.
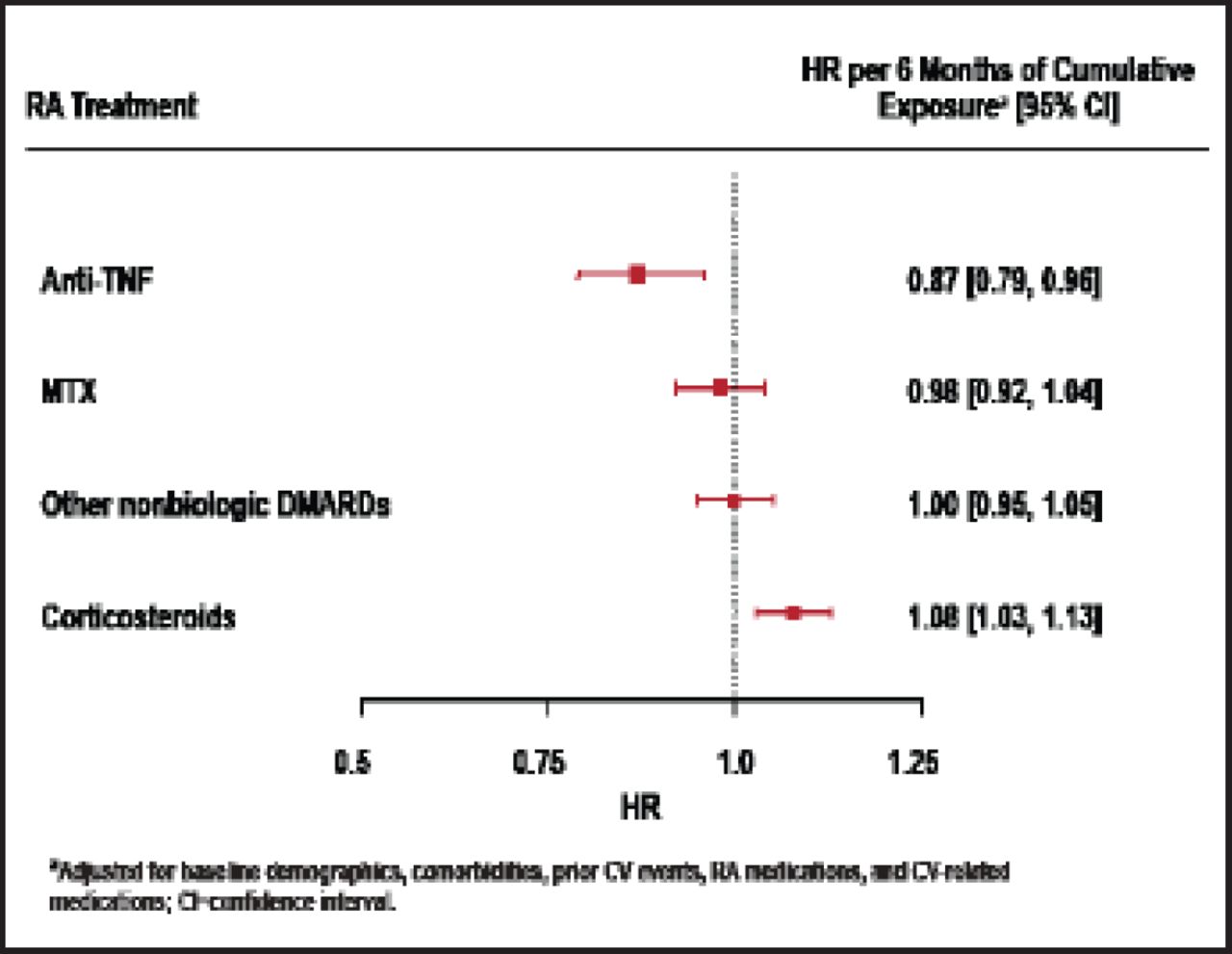
A total of 109,462 patients were assessed; of them, 1743 patients (1.6%) had at least 1 study CV event. In the multivariate regression model, each additional 6 months of anti-TNF therapy significantly reduced the risk for any study CV event. Patients who were treated with anti-TNF therapy had a hazard ratio (HR) of 0.87 (95% CI, 0.79 to 0.96; p=0.005) for the composite CV event endpoint compared with 0.98 (95% CI, 0.92 to 1.04) in patients who were treated with methotrexate, 1.00 (95% CI, 0.95 to 1.05) in patients who were treated with other nonbiologic DMARDs, and 1.08 (95% CI, 1.03 to 1.13) in patients who were treated with corticosteroids (Figure 1). The multivariate regression model predicted that cumulative use of anti-TNF therapy would result in a 24% reduction in CV events at 1 year, 42% reduction at 2 years, and 56% reduction at 3 years compared with not using anti-TNF therapy, adjusting for background use of methotrexate or other nonbiologic DMARDs.

HRs for Composite CV Event by RA Treatment.
Reproduced with permission from M. Nurmohamed, MD.
Each additional 6 months of anti-TNF therapy was associated with CV risk reduction in patients aged ≥50 years (HR, 0.86; 95% CI, 0.77 to 0.96; p=0.007). Risk reduction in methotrexate-naïve patients (HR, 0.85; 95% CI, 0.73 to 0.98; p=0.022) was similar to that observed in the total population. The hazard ratios for individual CV events in patients who were treated with anti-TNF drugs were 0.80 (95% CI, 0.67 to 0.95) for MI; 0.99 (95% CI, 0.86 to 1.16) for stroke, 0.76 (95% CI, 0.63 to 0.91) for unstable angina, and 0.78 (95% CI, 0.67 to 0.91) for CHF.
These results build on the findings of existing studies that have shown statistically significant CV risk reduction that was associated with anti-TNF therapy in RA patients (Table 1). Limitations of this study include the retrospective design, with the potential for unobserved confounding variables. In addition, clinical variables, such as lipid levels, blood pressure, and smoking status, were not available. The analysis adjusted for CV risk factors at baseline, including prior inpatient CV events, history of comorbidities, and CV-related medications.
Findings Support Existing Studies.
Longer exposure to anti-TNF therapy was associated with a greater reduction in the risk of CV events, primarily myocardial infarction, unstable angina, and congestive heart failure. Risk reduction was also observed in older patients and in methotrexate-naïve patients. Risk reduction was not observed for cumulative exposure to methotrexate or nonbiologic DMARDs.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.