

Summary
This article discusses the pathophysiological links between diabetes and heart failure (HF), treatment of diabetes to prevent HF, and treatment of diabetes in patients with HF.
- Diabetes Mellitus
- Heart Failure
Michael R. MacDonald, MD, Golden Jubilee National Hospital, Glasgow, Scotland, United Kingdom, discussed the pathophysiological links between diabetes and heart failure (HF), treatment of diabetes to prevent HF, and treatment of diabetes in patients with HF.
The RESOLVD substudy included 663 patients with HF, 27% of whom were known to have diabetes. Of those thought to be non-diabetic, 11% had diabetes, 12% had impaired glucose tolerance, and 34% had insulin resistance [Yan RT et al. Am J Cardiol 2005]. The Framingham study reported a substantially increased risk of HF in patients with diabetes.
Pathophysiological Links
Numerous studies have shown that diabetes is an independent predictor of worse prognosis in patients with HF. Conversely, HF worsens the prognosis in patients with diabetes [Bertoni HG et al. Diabetes Care 2004]. Additionally, diabetes and HF can each lead to the other condition. Insulin resistance is common in patients with HF and is independent of HF etiology; it predicts incident HF, reduced functional capacity, more severe symptoms, and reduced survival [Doehner W. J Am Coll Cardiol 2008]. At the time of diabetes diagnosis, 40% of patients have macroangiopathy, 40% have albuminuria, 15% have retinopathy, 50% have hypertension, and 50% have hypertriglyceridemia [Meeuwisse-Pasterkamp SH et al. Expert Rev Cardiovasc Ther 2008]. Possible mechanisms for insulin resistance in HF include age, genetic factors, diet and decreased exercise, endothelial dysfunction, impaired tissue performance, oxidative stress, and humoral factors [Doehner W. J Am Coll Cardiol 2008]. Several studies have demonstrated evidence for a diabetic cardiomyopathy. The CHARM study reported an increased incidence of cardiovascular (CV) death or hospitalization due to HF (p=0.0009) and hospitalization due to HF (p=0.0029) in patients with diabetes versus those without diabetes [MacDonald MR et al. Eur Heart J 2008].
Treatment of Diabetes and HF
The CHARM study showed that increasing HbA1C is a progressive risk factor for CV death, worsening HF, and death. Results of observational studies are inconsistent, however, and no randomized trials have evaluated the effect of reducing HbA1C on HF outcomes.
A case-control study showed that metformin is the only diabetes drug that improves outcomes in patients with diabetes and HF [MacDonald MR et al. Diabetes Care 2010]. Sulfonylureas increase insulin release but promote fluid retention and can cause hypoglycemia. Insulin therapy is associated with a higher incidence of HF, as are thiazolidinediones.
Glucose-like peptide-1 (GLP-1) receptors are present in myocardium, and GLP-1 mimetics may have benefits in HF. They may alter substrate utilization and have beneficial effects on endothelium. GLP-1 mimetics have an inotropic effect in animals. In addition, a study in 12 HF patients showed that the GLP-1 mimetic exenatide improved ejection fraction, maximal O2 uptake, 6-minute walk test, and quality of life.
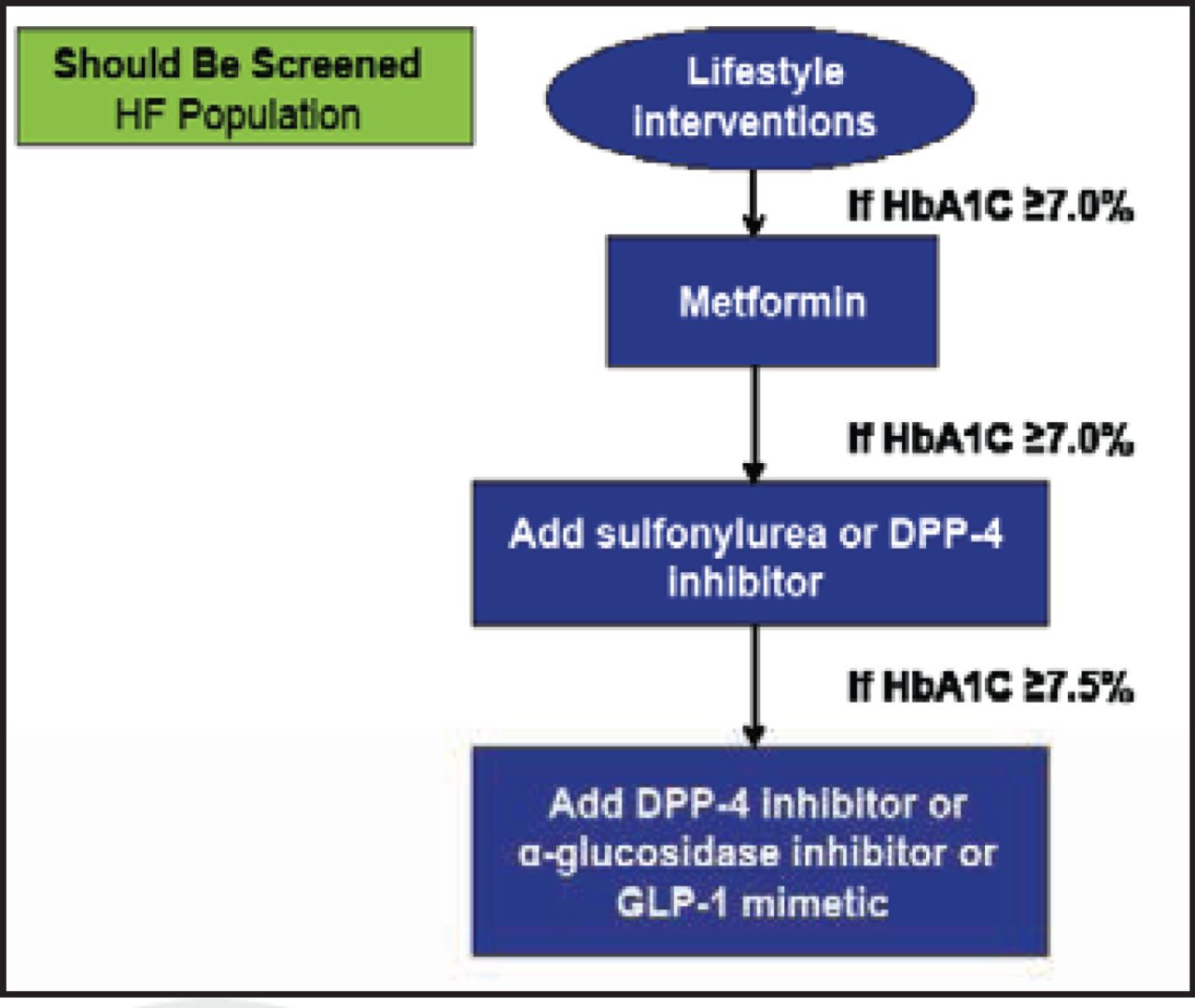
Dr. MacDonald proposed a glycemic control strategy beginning with lifestyle interventions, followed by the addition of metformin, sulfonylurea or dipeptidyl peptidase-4 (DPP-4) inhibitor, and a DPP-4 inhibitor or an a-glucosidase inhibitor or a GLP-1 mimetic (Figure 1).

Glycemic Control Strategy.
Reproduced with permission from MR MacDonald, MD.
Patients with diabetes often develop HF, which places a substantial burden on healthcare resources. Diabetes appears to directly affect the myocardium, but pathophysiologic data for humans are not available. HF patients should be screened for diabetes. Prospective studies examining therapeutic strategies in patients with diabetes and acute or chronic HF are warranted.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.