

Summary
The global magnitude of blindness from diabetic retinopathy (DR) is daunting. In 2010, the World Health Organization (WHO) reported 586,004 cases worldwide [WHO Prevention of Blindness and Visual Impairment: 2010], with the highest numbers of visual impairment and blindness in Southeast Asia. This article discusses global challenges and opportunities in the treatment of DR.
- Retinal Diseases
- Prevention & Screening
- Diabetes Mellitus
The global magnitude of blindness from diabetic retinopathy (DR) is daunting. In 2010, the World Health Organization (WHO) reported 586,004 cases worldwide [WHO Prevention of Blindness and Visual Impairment: 2010], with the highest numbers of visual impairment and blindness in Southeast Asia. Barbara E.K. Klein, MD, University School of Medicine and Public Health, Madison, Wisconsin, USA, discussed global challenges and opportunities in the treatment of DR.
DR is the fifth most common cause of blindness, with rates varying by geographic region. In China, an estimated 92.4 million people had diabetes in 2010, which is 4.5 times the number that was estimated in the Chinese National Nutrition and Health Survey in 2002 [Yang W et al. N Engl J Med 2010]. In sub-Saharan Africa, an estimated 12.1 million people had diabetes in 2010, and that figure is expected to double by 2030 [Tuei VC et al. Diabetes Metab Res Rev 2010]. Approximately 15% of people with diabetes in sub-Saharan Africa have severe retinopathy.
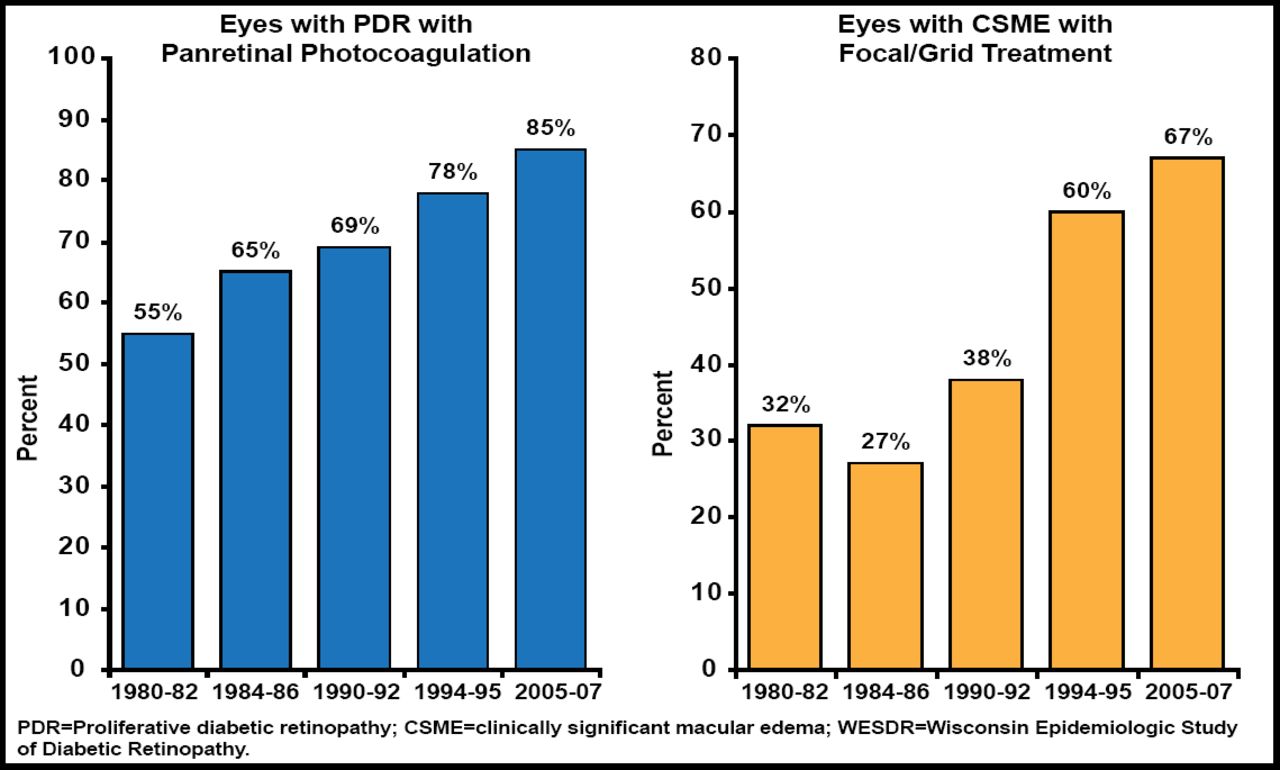
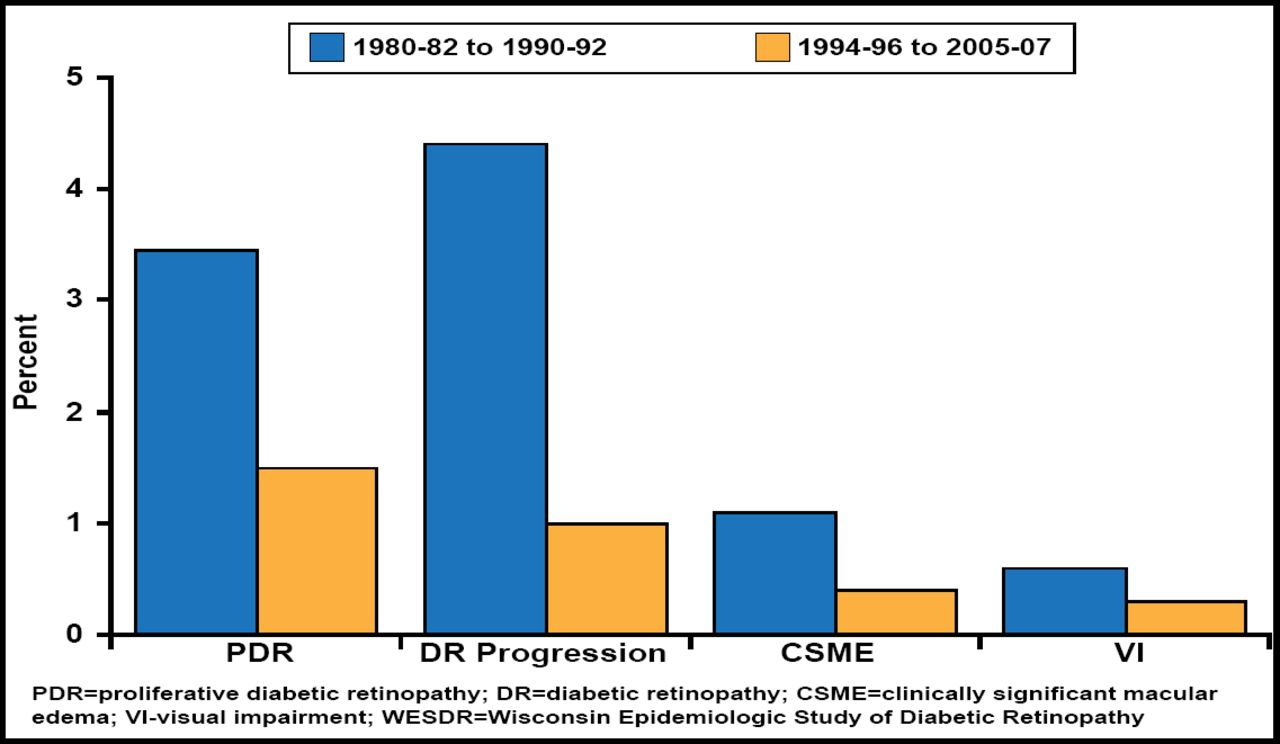
In the population-based Wisconsin Epidemiologic Study of Diabetic Retinopathy in persons with type 1 diabetes, there was a trend toward increasing rates of treatment for proliferative DR and clinically significant macular edema (Figure 1), with declines in estimated annual incidence (Figure 2) [Klein R, Klein BE. Diabetes 2010]. Data on type 2 diabetes from the National Health and Nutrition Examination Survey 2005–2008 also indicate a lower prevalence of diabetic eye diseases than previously reported [Klein R, Klein BE. Diabetes 2010].

Treatment Trends in PDR and CSME in Persons with Type 1 Diabetes in the WESDR.
Reproduced with permission from the American Diabetes Association. Klein R and Klein BB. Diabetes 2010.

Estimated Annual Incidence of PDR, Progression of DR, Incidence of CSME, and Incidence of VI in Persons With Type 1 Diabetes in the WESDR.
Reproduced with permission from the American Diabetes Association. Klein R and Klein BB. Diabetes 2010.
Although new findings suggest that rates of severe DR are falling in the United States, changes in the prevalence and quality of health care vary from country to country. Thus, interventions must be flexible. Resources that are needed include: programs to identify people with diabetes in many locations around the world; adequate healthcare and social services to ensure careful evaluation of each case; and the personnel and budget for follow-up care [Aspelund T et al. Diabetologia 2011].
Experience shows that effective screening for DR in patients with diabetes requires: regional centers or mobile examination/photography units; computer/internet access; resources for follow-up; personnel and technical equipment for treatment; and a communication system for practitioners and patients for education.
Data show that digital photography with telemedicine links has the potential to deliver cost-effective screening to remote populations. Of techniques that had been used to identify DR, 3 dilated photos had the highest sensitivity and specificity compared with 7 standard field photographs [Prevention of Blindness from Diabetes Mellitus: Report of a WHO Consultation. Geneva, Switzerland, 9–11 November 2005]. Systematic screening yields lower costs for quality of life-years that are saved [Jones S, Edwards RT. Diabet Med 2010].
According to Dr. Klein, the prevalence of diabetic retinopathy is likely to increase even in the presence of improved care because of increased longevity and a growing number of people who have diabetes. Prevention is the mission of research, but current efforts in the field will rely on adherence to known therapies to prevent or delay the onset of retinopathy and to develop improved methods to provide timely, affordable, and acceptable care.
- © 2012 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.