

Summary
It has been reported that ischemic postconditioning reduces infarct size in patients with ST-segment myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) [Staat P et al. Circulation 2005]. The objective of the Effects of Postconditioning on Myocardial Reperfusion [POST; NCT00942500] study was to evaluate the safety and efficacy of postconditioning in patients with STEMI undergoing primary PCI.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Myocardial Infarction
While it has been reported that ischemic postconditioning reduces infarct size in patients with ST-segment myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PCI) [Staat P et al. Circulation 2005], other trials have reported inconsistent results [Lonborg J et al. Circ Cardiovasc Interv 2010; Sorensson P et al. Heart 2010; Freixa X et al. Eur Heart J 2012; Tarantini G et al. Int J Cardiol 2012] and there have been no large-scale trials to date. The objective of the Effects of Postconditioning on Myocardial Reperfusion [POST; NCT00942500] study presented by Joo-Yong Hahn, MD, Samsung Medical Center, Seoul, Korea, was to evaluate the safety and efficacy of postconditioning in patients with STEMI undergoing primary PCI.
A total of 700 patients with STEMI undergoing primary PCI from 17 South Korean hospitals were randomized after diagnostic coronary angiography to primary PCI with postconditioning (n=350) or conventional primary PCI (n=350). Postconditioning consisted of 4 episodes of 1-minute balloon occlusion and 1-minute deflation immediately after restoration of coronary flow. Patients were treated with aspirin (300 mg) and clopidogrel (600 mg). The primary endpoint was complete ST-segment resolution (STR >70%) at 30 minutes after the procedure. The secondary endpoints were TIMI flow grade after PCI, myocardial blush grade (MBG), major adverse cardiac events (MACE; composite of death, reinfarction, severe heart failure, or stent thrombosis), MACE components, and target vessel revascularization at 30 days.
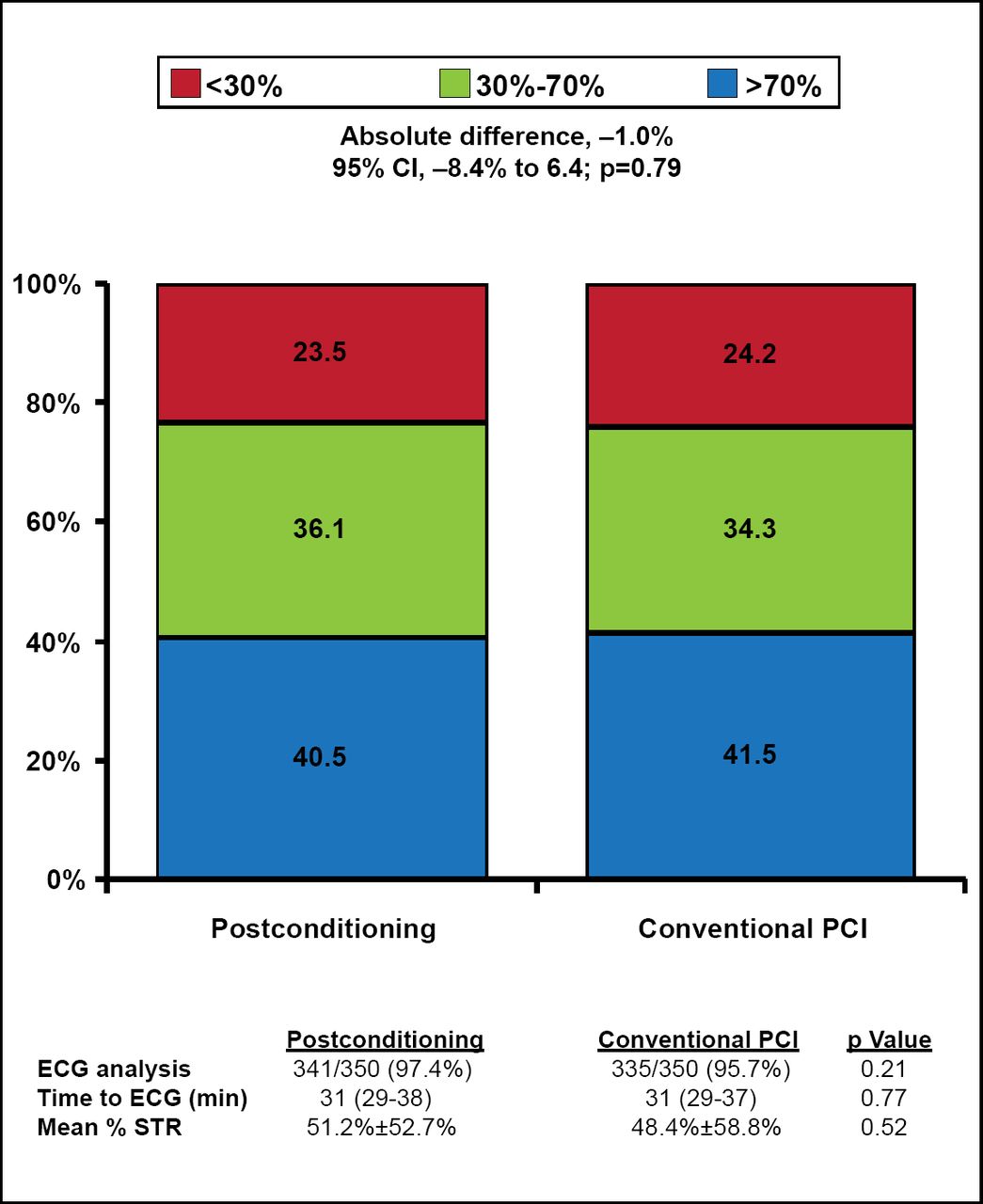
Patients' mean age was 60 and ∼75% were male. Baseline clinical characteristics and angiographic findings were well balanced between the 2 treatment groups. ECG was performed in 97.4% of postconditioning patients and 95.7% of conventional PCI patients (p=0.21). Time to ECG was 31 minutes in both groups (p=0.77). There was no significant difference in the primary endpoint (complete STR) for those patients who had postconditioning versus conventional PCI (40.5% vs 41.5%; 95% CI, −8.4% to 6.4%; p=0.79; Figure 1). The primary endpoint results were consistent across prespecified subgroups.

Primary Endpoint: Complete ST-Segment Resolution.
Reproduced with permission from JY Hahn, MD.
There was no significant difference in TIMI flow grade (p=0.08) or MBG (p=0.20) after PCI with postconditioning versus conventional PCI. Clinical outcomes at 1-month after PCI were not significantly different between the 2 groups (Table 1). STR <30, MBG of 0/1, and postprocedural TIMI flow grade of 0/1 were significantly associated with higher rates of mortality and MACE.
Clinical Outcomes at 1 Month.
The study had several limitations. Providers were not blinded to treatment allocation, the study was underpowered for clinical outcomes, postconditioning was not performed per protocol in ∼8% of patients, and ECGs before and 30 minutes post-procedure were not available in 3.5% of patients. Patients with hemodynamic instability, cardiogenic shock, or a left main lesion who might have had lethal reperfusion injury and received potential benefit from postconditioning were excluded.
The investigators concluded that ischemic postconditioning with primary PCI did not improve myocardial reperfusion compared with conventional primary PCI. Clinical outcomes at 1 month were not significantly different between 2 groups. A cardioprotective effect of ischemic postconditioning was not observed in any of the prespecified subgroups.
- © 2012 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.