

Summary
Timing has long been recognized as the most crucial aspect in the care of people with ST-segment elevation myocardial infarction (STEMI). A session on state-of-the-art STEMI care provided an opportunity to discuss the influence of ischemia time and explore ways to improve treatment quality with organized systems of care.
- Cerebrovascular Disease
- Myocardial Infarction
Timing has long been recognized as the most crucial aspect in the care of people with ST-segment elevation myocardial infarction (STEMI). A session on state-of-the-art STEMI care provided an opportunity to discuss the influence of ischemia time and explore ways to improve treatment quality with organized systems of care.
Effect of Time on Ischemia
Studies suggest that delays to reperfusion increase infarct size and reduce myocardial salvage in patients with STEMI [Francone M. J Am Coll Cardiol 2009]. However, data are conflicting about the significance of onset-to-balloon time, with one study showing a significant association between the development of a transmural infarct but not infarct size [Hahn JY. Am J Cardiol 2008] and another indicating that salvaged myocardium is markedly reduced when reperfusion occurs more than 90 minutes after coronary occlusion [Francone M. J Am Coll Cardiol 2009].
The first 2 to 3 hours after symptom onset are most important, said Holger Thiele, MD, University of Leipzig Heart Center, Leipzig, Germany, who led a panel discussion on optimal cutoff time for treatment of ischemic events. All panelists agreed that assessing ischemia time is challenged by the subjectivity of patient recall and reporting.
Christopher Granger, MD, Duke Clinical Research Institute, Durham, North Carolina, USA, also discussed the timing of primary percutaneous coronary intervention (PCI). The American College of Cardiology/American Heart Association (ACC/AHA) guidelines recommend primary PCI as the preferred strategy only if it can be done within 90 minutes of first medical contact. If the time is expected to be longer than that, fibrinolytic therapy within 30 minutes of hospital presentation is the preferred perfusion method.
According to Dr. Granger, the most compelling data for life-saving reperfusion treatment comes from fibrinolytic therapy. “Here, we know that regardless of the window of ischemia time, we can get survival benefit from reperfusion therapy within 12 hours of symptom onset,” he said, adding that studies indicate a greater degree of benefit with earlier administration of fibrinolytic therapy. “Survival improves with earlier treatment, and it's not incremental—the shorter the time, the better. We should be providing the fastest reperfusion therapy we can,” he said, citing newer fibrinolytic agents that help improve outcomes.
In discussing delay to PCI that is expected to be longer than the guideline-recommended time, the panel explored the question of whether it is better to give fibrinolytic therapy immediately or to transfer the patient, with some delay, to a PCI center. The panelists agreed that this continues to be an important question, with no well-defined answer. They also agreed that although the data support either a PCI-directed strategy when available in a timely fashion or a fibrinolytic strategy when PCI is not available instead of a routine facilitated PCI strategy, what the patient receives before PCI is a key unanswered question.
Systems of Care
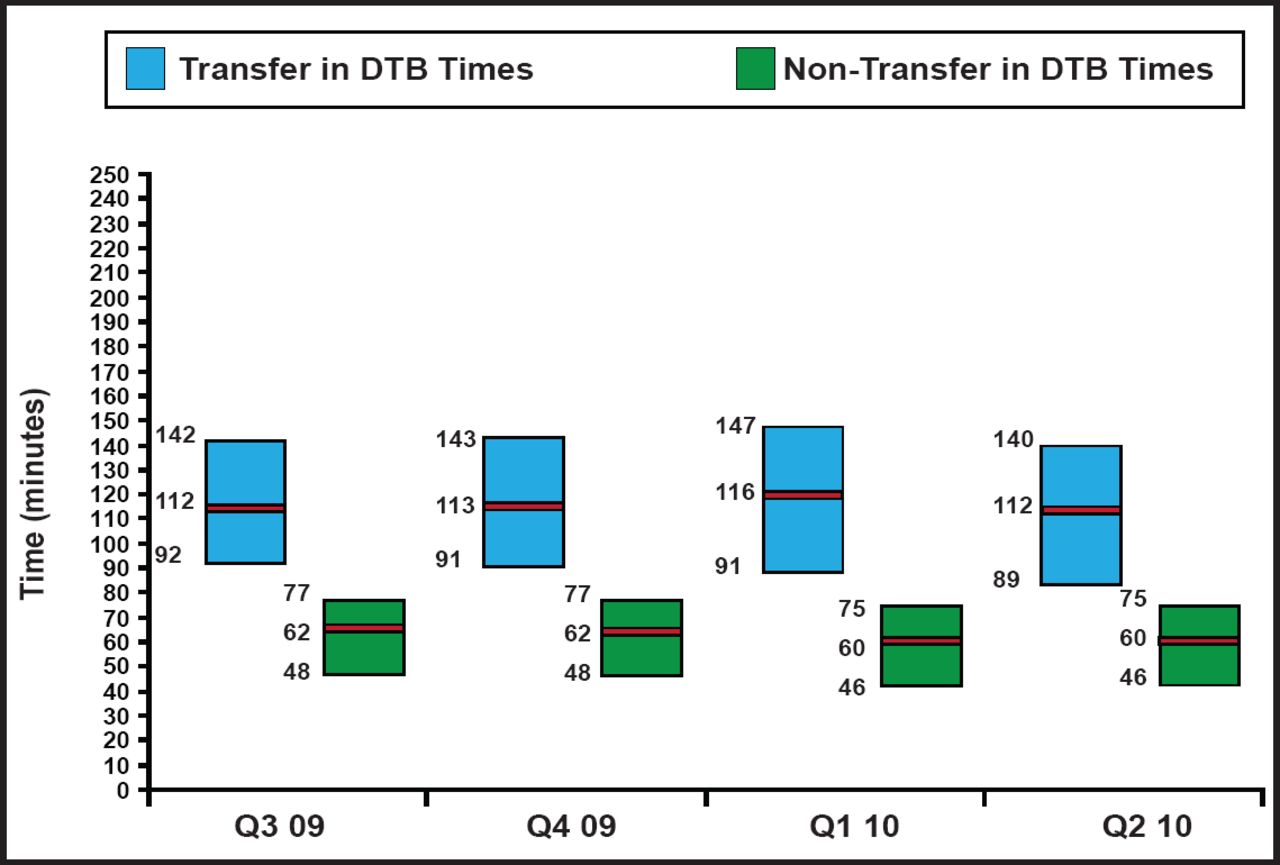
Comprehensive systems of care are critical for improving the time-to-reperfusion therapy for patients with STEMI. Programs, such as the ACTION Registry-Get with the Guidelines (GWTG) and the AHA's Mission: Lifeline, have started to close the gap between ideal and actual time. Several studies have found significant improvements in door-to-balloon times when comprehensive systems of care are in place (Figure 1). Door-to-balloon times that are associated with transfers to PCI-capable facilities have also decreased, but the rates of ideal timing are far lower than in cases when no transfer is necessary. System delays have a definite influence on outcomes; long delays in transporting patients to a PCI-capable facility are associated with higher 7-year mortality.

STEMI DTB Times.
DTB=door-to-balloon time. Reproduced with permission from C. Granger, MD.
Despite the success of better times to reperfusion, no study has yet to show improvements in mortality, said Alice K. Jacobs, MD, Boston University Medical Center, Boston, Massachusetts, USA. “This is the challenge,” she noted.
In addition to the need to improve the timing of transfers, prehospital diagnosis of STEMI also has to be better than it is. Studies in both urban and rural settings show that a prehospital diagnosis of STEMI with direct admission to a PCI center saves time and improves outcomes. A recent report from Denmark showed that prehospital electrocardiographic (ECG) diagnosis and direct referral for primary PCI enables STEMI patients who live far from a PCI center to achieve a system delay comparable with that of patients who live in close proximity to a PCI center [Sorenson JT et al. Eur Heart J 2011].
Although many studies have shown that transmitting ECG readings is not essential for improving timing, James McCarthy, MD, Memorial Hermann–Texas Medical Center Hospital, Houston, Texas, USA, said that the prehospital ECG is an essential piece of the puzzle. Methods of transmitting ECG readings to hospitals are improving, and medical centers can enhance their systems of care by providing multiple means of communication, such as through cell phones and dedicated receivers. Dr. McCarthy noted that “Emergency medical personnel need to know that the ECG is the first thing to do; the history can be taken later.” Prehospital activation can save 15 minutes; yet, ECG is not done in the field in many parts of the country, and even when it is, there are tremendous disparities in who receives it, he said.
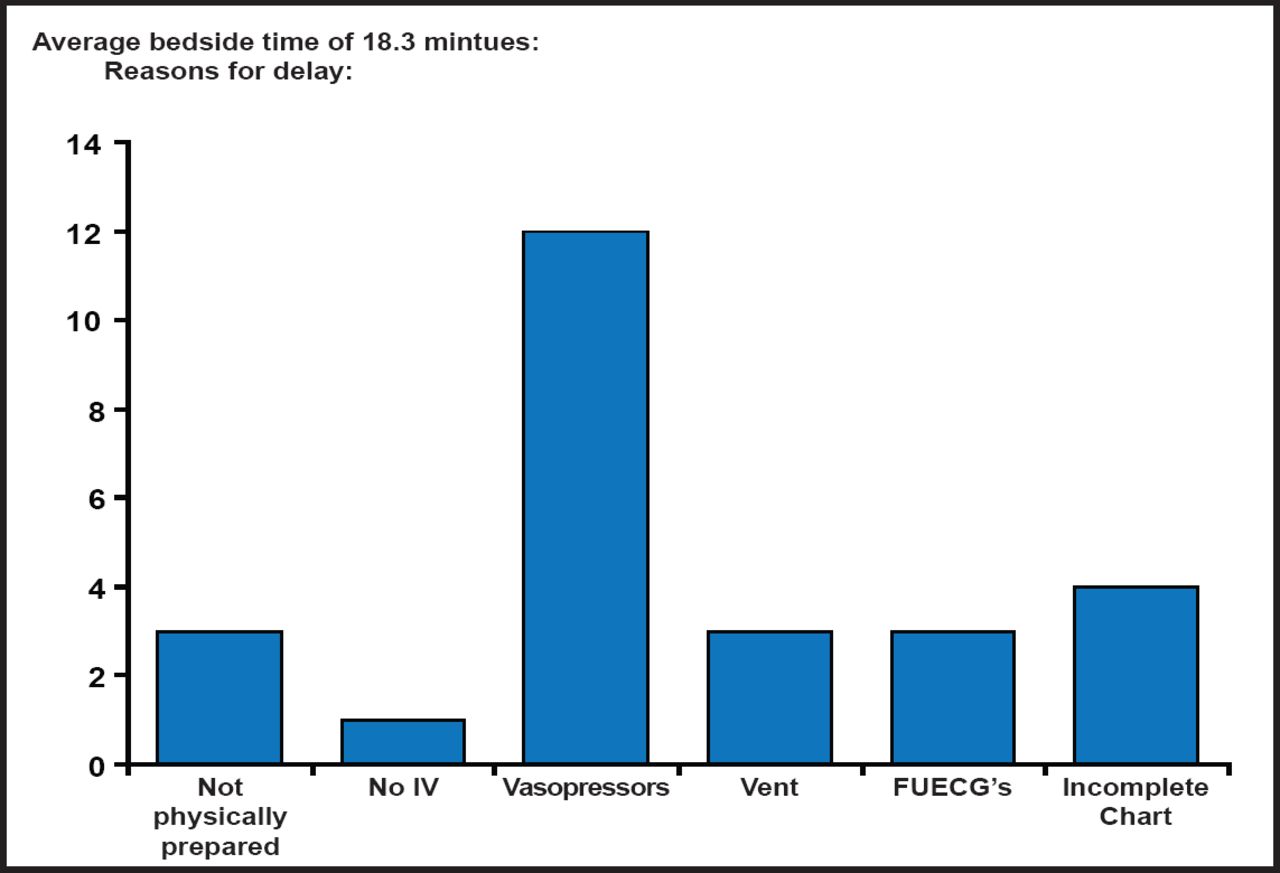
Other integral components of an efficient system of care include established medical and transport protocols and simplified handoff sheets for emergency medical personnel and transferring facilities. A recent study of air transfer found that the need for the transport team to initiate vasopressor therapy was the most frequently cited reason for delay in liftoff to the receiving facility (Figure 2) [McGrath CP et al. Air Med J 2010]. “Drips are the Achilles heel of transfers,” Dr. McCarthy said, explaining that the types of pumps that are used to administer vasopressors differ between units, making it necessary to discontinue the drip and reload the drug. He said that the reported average time to do this is 18 minutes.

Analysis of Transfer Delays.
Reprinted from Air Med J. McGrath CP et al. March-April 2010;29(2):84–87. With Permission from Elsevier.
Dr. Granger strongly encouraged attendees to use the ACTION Registry-GTWG and AHA tools to benchmark their performance. “If you don't measure it, you can't improve it,” he said. He also said that hospitals should ensure that all staff members know the record of times and that these figures are reported to other hospitals and emergency medical services. Educating emergency medical personnel about why early diagnosis of STEMI is essential can help them become more engaged in identifying ways to improve timing.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.