

Summary
In patients with newly diagnosed type 2 diabetes mellitus (T2DM), complications are often present at the time of diagnosis, suggesting that clinical onset of the disease occurred years prior to diagnosis [Koopman RJ et al. Ann Fam Med 2006]. This article discusses the prevalence of metabolic risk among individuals with defined metabolic risk factors and T2DM and shared results from the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes [SHIELD] study.
- Cardiometabolic Disorder
- Diabetes Mellitus
- Prevention & Screening
An estimated 25.6 million adults in the United States (US) have diabetes mellitus [Centers for Disease Control and Prevention, Prevalence of diagnosed diabetes among adults aged 18 years and over: United States, 1997–2010, 2011]. In patients with newly diagnosed type 2 diabetes mellitus (T2DM), complications are often present at the time of diagnosis, suggesting that clinical onset of the disease occurred years prior to diagnosis [Koopman RJ et al. Ann Fam Med 2006]. Harold Bays, MD, Louisville Metabolic and Atherosclerosis Research Center, Louisville, Kentucky, USA, discussed the prevalence of metabolic risk among individuals with defined metabolic risk factors and T2DM and shared results from the Study to Help Improve Early evaluation and management of risk factors Leading to Diabetes (SHIELD) study.
SHIELD was a 5-year longitudinal observational study of individuals with or at risk for diagnosis of diabetes mellitus. Following an initial screening phase, follow-up questionnaires were mailed to a stratified random sample of individuals (n=22,001) with type 1 or type 2 diabetes or at high (3 to 5 American Diabetes Association risk factors) or low (0 to 2 risk factors) risk for diabetes [Clark NG et al. Diabetes Care 2007]. The population-based survey was designed to better understand the risk for the development of diabetes mellitus, as well as the disease burdens that are associated with it. The study sample was representative of the United States population with respect to age, gender, geographic region, household size, and income. Year-to-year from 2005–2009, the response rate to SHIELD (a survey-only study) was 68% to 80%. Outcomes were compared with 1999–2002 National Health and Nutrition Examination Survey (NHANES; a study that involved surveys and laboratory confirmation).
While the prevalence of diabetes mellitus (8% in SHIELD and 9% in NHANES; p<0.01) and hypertension (23% in SHIELD and 29% in NHANES; p<0.01) was similar, dyslipidemia was reported only half as frequently in SHIELD (26%) than in NHANES (53%; p<0.01). Components of dyslipidemia were also uniformly lower in SHIELD than NHANES: high triglycerides (TG)=17% versus 35%; high low-density lipoprotein cholesterol=10% versus 14%; high TG=7% versus 17%; and low high-density lipoprotein cholesterol= 5% versus 24% (p<0.01 for all). The self-reported nature of SHIELD likely accounted for this difference when compared with NHANES [Bays HE Curr Med Res Opin 2008].
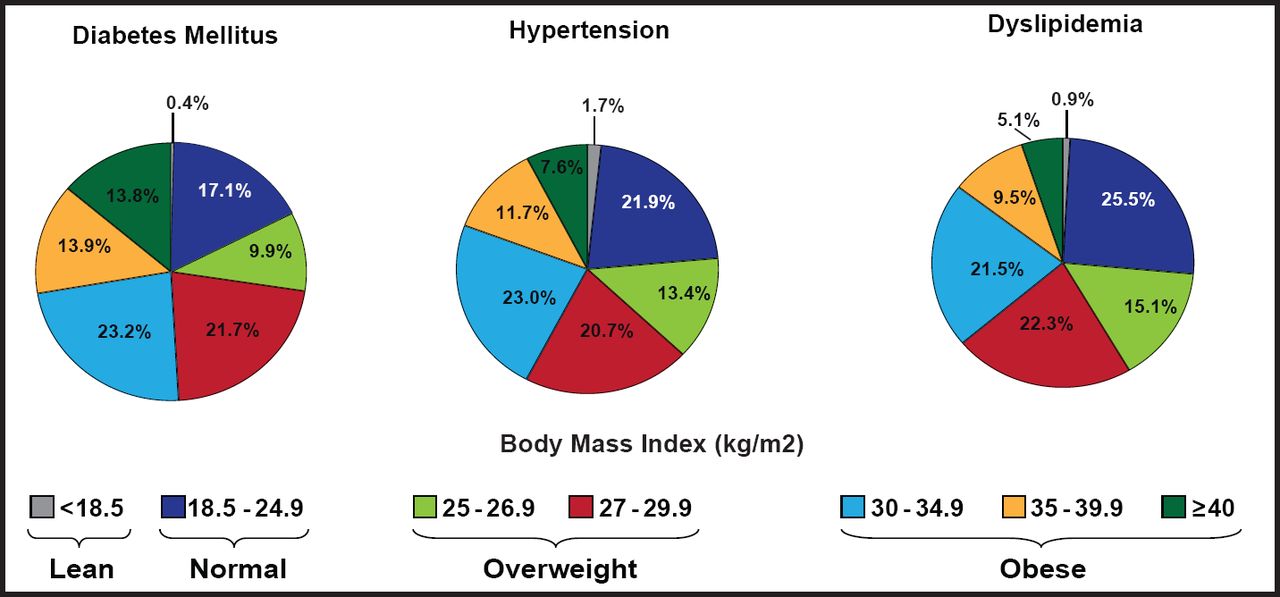
Individuals with diabetes or cardiometabolic risk factors and body mass index (BMI) ≥28 kg/m2 are considered at high risk [Green AJ et al. Int J Clin Pract 2007]. According to Dr. Bays, NHANES 1999–2002 results showed that among patients with diabetes mellitus, 21.7% had a BMI of 27 to 29.99 kg/m2 (overweight) and 50.9% had a BMI >30 kg/m2 (obese; Figure 1) [Bays HE et al. Int J Clin Pract 2007; Bays HE et al. Am J Med 2009].

BMI Distribution Among Patients with Metabolic Diseases.
Reproduced with permission from Excerpta Medica Inc., from “Sick Fat,” Metabolic Disease, and Atherosclerosis 2008, Bays HE et al, vol. 122 no. 1: S27-S37; permission conveyed through Copyright Clearance Center, Inc.
Metabolic diseases often have the unified underlying pathophysiological process of adiposopathy or “sick fat.” This may help explain why the distributions of BMI for diabetes mellitus, hypertension, and dyslipidemia are generally similar.
The obesity epidemic contributes to the increasing prevalence of high blood sugar, high blood pressure, and dyslipidemia [Bays HE. Am J Med 2009]. SHIELD respondents at high-risk or and those with T2DM (>46%) received recommendations to change their lifestyle habits (increase exercise and change eating habits) compared with 29% of low-risk respondents (p<0.0001). Although T2DM and high-risk respondents reported attitudes and knowledge that were conducive to good health, the majority did not translate these positive traits into healthy behavior with respect to diet, exercise, and weight loss [Green AJ et al. Int J Clin Pract 2007].
Clinical and Health Care Policy Implications
James R. Gavin, III, MD, PhD, Emory University School of Medicine, Atlanta, Georgia, USA, discussed the clinical and health care policy implications for management of diabetes and individuals who are at risk, based on findings from the SHIELD study.
Largely because of the pathogenic potential of excess adipose tissue, an increase in body fat is generally associated with heightened risk of metabolic diseases, such as T2DM [Bays HE et al. Int J Clin Pract 2007]. SHIELD outcomes pointed to a need to identify gaps in the treatment of obesity; increase advice to low-risk individuals on therapeutic lifestyle changes; and provide practical, patient-friendly self-management tools for those with T2DM.
Dr. Gavin stressed the need for informed and empowered patients—those with the motivation, skills, and confidence to effectively make decisions about and manage their health. He cited a need for more education and outreach to promote active self-management with accessible, easy-to-use tools. He also called for enhanced peer support/interaction and communication between patients and health care providers (eg, through cell phones, web portals, and wellness coaches).
Because the majority of SHIELD respondents was aware of healthy behaviors but failed to engage in them, Dr. Gavin recommended more support for diabetes educators and health care providers to assist them in teaching patients how to make healthy choices using public policy as a tool (eg, pay for performance). He suggested that data on attitudes/behaviors from SHIELD be used in developing the approach and content of group visits and creating effective surrogates for health care visits, since increased frequency of contact translates into better adherence and outcomes.
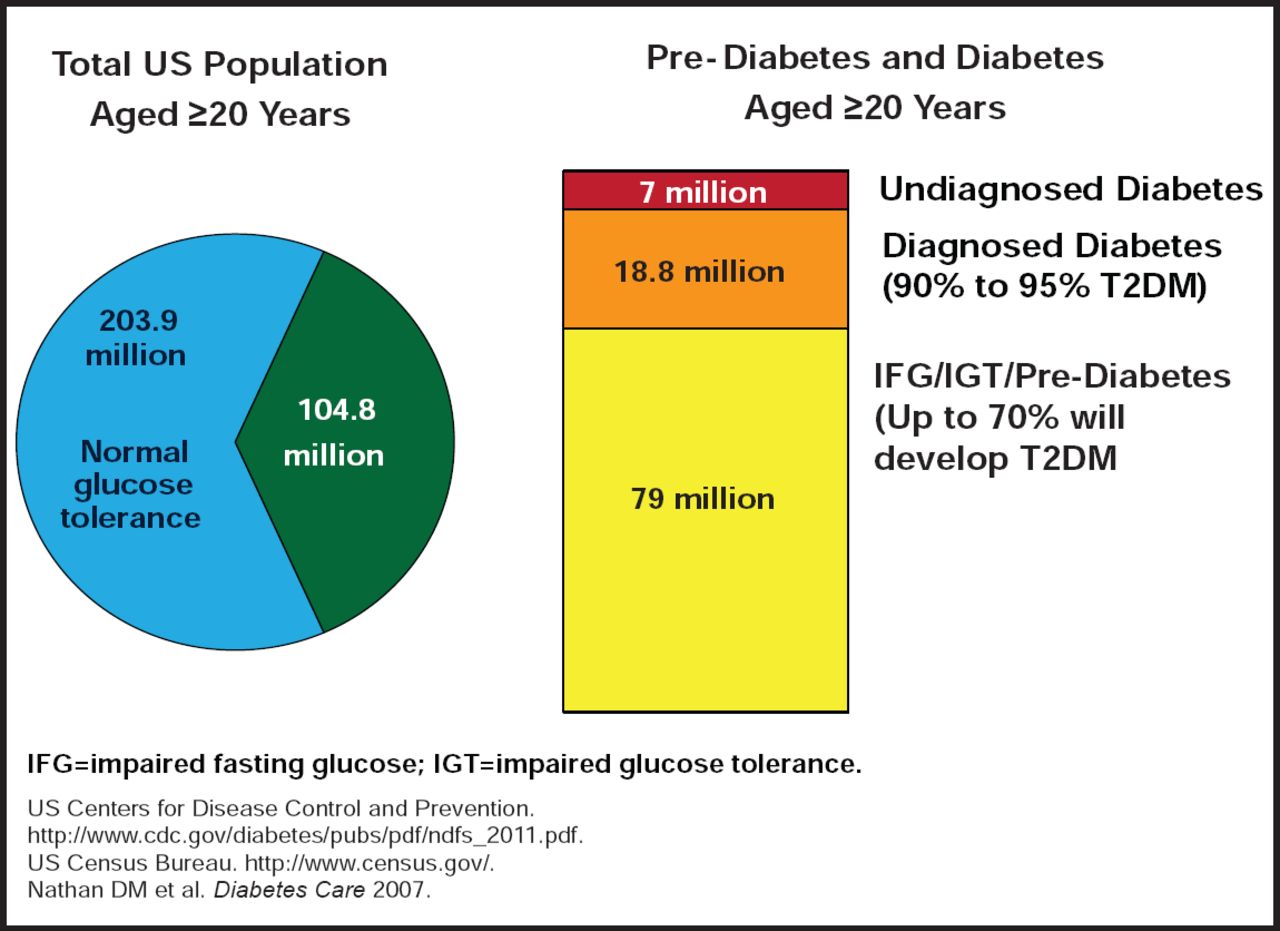
Diabetes and prediabetes are common in the US [Nathan DM et al. Diabetes Care 2007] (Figure 2)— factors with implications for risk assessment include:
-
Use of SHIELD data to more accurately identify within-group predictors of risk progression
-
Linking of available prevention tools to indications of increased risk for progression
-
Use of patient-measured parameters to derive risk predictors of sufficient rigor
-
Enhanced linking of attitudes and behaviors to risk in patient-centered ways
-
Strengthening of current screening tools

Diabetes and Prediabetes in the US.
The SHIELD study indicated a need to consider cardiometabolic risk and factors beyond type T2DM in prediction models. These include demographics (eg, prescription drug coverage, geographic region, ethnicity); diabetes symptoms (eg, irritability, “high sugar,” gestational diabetes); lifestyle (eg, exercise, health, and smoking status); and medical conditions (eg, COPD, circulation problems, arthritis, asthma).
Clinical and health care implications range from actions that are taken by primary care physicians before patients develop T2DM to assessment of how SHIELD outcomes can be used to improve screening beyond the disease. Consideration needs to be given to what health policies should be implemented to reduce the epidemic—eg, outreach efforts, use of social media; what role endocrinologists and cardiologists should play in identifying at-risk individuals; and how we can better leverage new insights into public attitudes and behaviors.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.