

Summary
This article outlines 12 concepts to improve door-to-balloon time and clinical outcomes using data from the SINCERE Database [S. Mehta. Textbook of STEMI Interventions] and actual clinical experiences performing ST-segment elevation myocardial infarction.
- interventional techniques & devices
- myocardial infarction
Using data from the SINCERE Database [S. Mehta. Textbook of STEMI Interventions] and his extensive experience performing ST-segment elevation myocardial infarction (STEMI) interventions, Sameer Mehta, MD, University of Miami, Miami, Florida, USA, outlined 12 concepts to improve door-to-balloon (D2B) time and clinical outcomes.
Current understanding regarding D2B is the shorter the time, the better the outcome, similar to earlier observations with fibrinolytic therapy. A significant mortality benefit is noted when reperfusion therapy with either percutaneous coronary intervention (PCI) or lysis occurs within the first 2 to 3 hours after symptom onset. If presentation is late after symptom onset, there is little mortality benefit from earlier patency with fibrinolytic therapy, and patients may be subject to the bleeding risks and increased rates of early rupture that are associated with fibrinolytic drugs [Gersch BJ et al. JAMA 2005]. Thus, current guidelines recommend PCI over fibrinolytic therapy when there are longer delays between symptom onset and presentation.
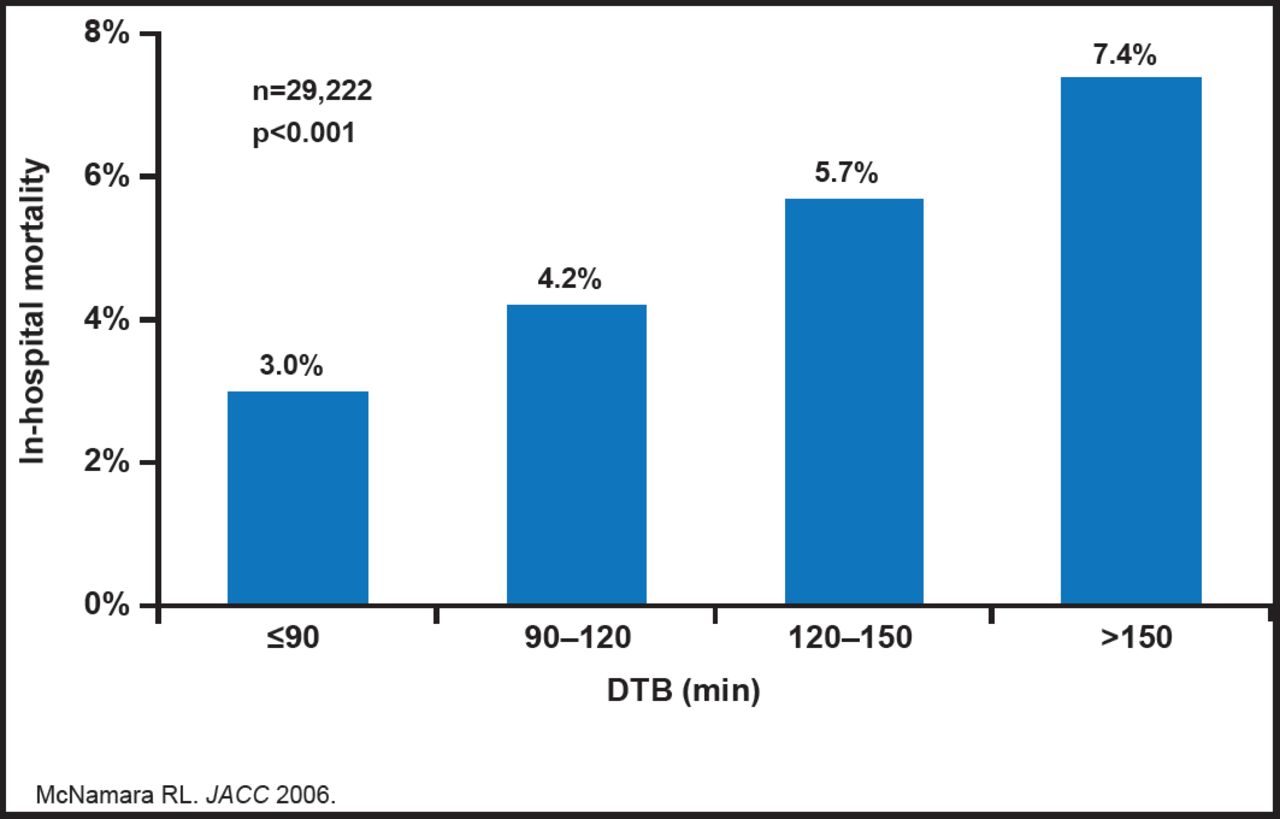
Longer D2B times are associated with increased in-hospital mortality (3.0%, 4.2%, 5.7%, and 7.4% for D2B times of ≤90 min, 91 to 120 min, 121 to 150 min, and >150 min, respectively; p<0.01 for trend). Time to primary PCI is strongly associated with mortality risk and is important, regardless of time from symptom onset to presentation and regardless of baseline risk of mortality (Figure 1) [McNamara RL et al. J Am Coll Cardiol 2006]. Guidelines recommend that the interval between arrival at the hospital and D2B time during primary PCI should be ≤90 minutes and, if not possible (eg, non-PCI-capable facility), then other mechanisms of reperfusion, such as fibrinolysis should be used. However, few hospitals meet this objective.

D2B Times.
Reproduced with permission S. Mehta, MD.
Several specific hospital strategies that are associated with a significant reduction in the D2B time in the management of STEMI have been identified by Bradley EH et al. [New Engl J Med 2006]. They include having emergency medicine physicians activate the catheterization laboratory (mean reduction in D2B time, 8.2 minutes), having a single call to a central page operator activate the laboratory (13.8 minutes), having the emergency department activate the catheterization laboratory while the patient is en route to the hospital (15.4 minutes), expecting staff to arrive in the catheterization laboratory within 20 minutes (vs >30 minutes) after being paged (19.3 minutes), having an attending cardiologist always on site (14.6 minutes), and having staff in the emergency department and the catheterization laboratory use real-time data feedback (8.6 minutes). Despite the effectiveness of these strategies, only a minority of hospitals that were surveyed were using them.
With this knowledge in mind, Dr. Mehta presented 12 basic, hard-learned concepts to improve STEMI care.
-
Many cases occur in the early morning hours, and some patients have no insurance. Accept this and move on.
-
Always consider the driving times to the various feeder hospitals in the area. Traffic can be an issue.
-
Who should be performing these procedures? Someone who is dedicated to this will require lifestyle changes. The individual will be challenged by the logistics that are associated with an extremely time-sensitive procedure and the unpredictable.
-
Break STEMI management into procedure and process (Table 1).
-
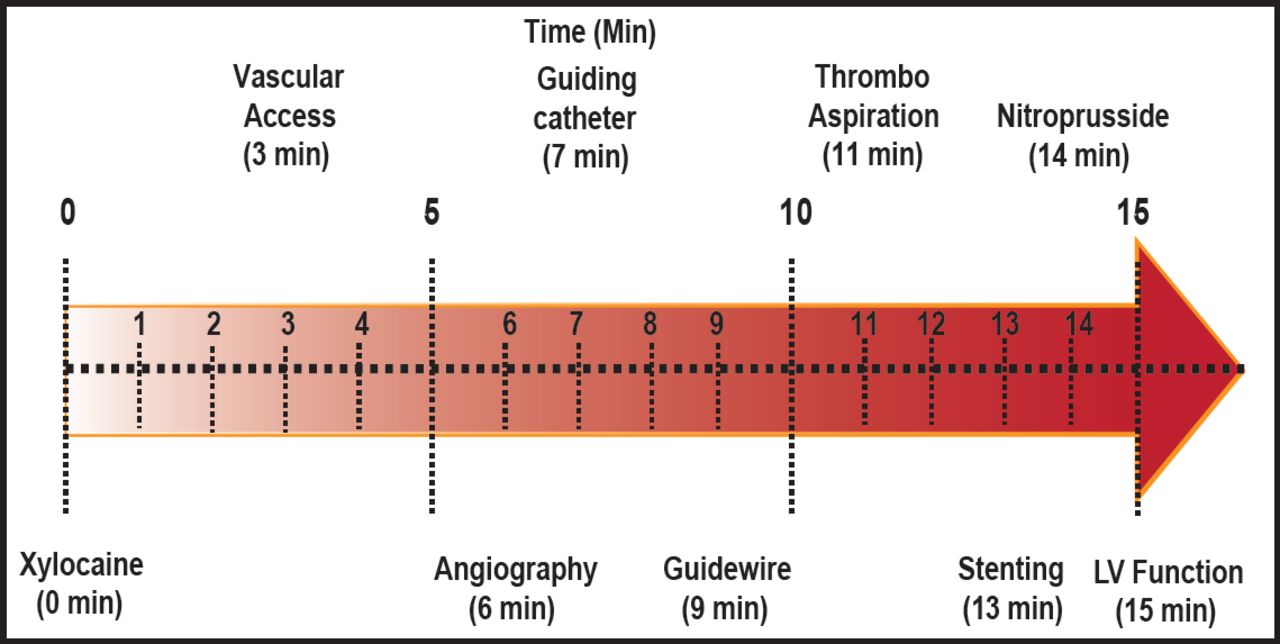
Standardized technique to improve efficiency and outcomes. Fifteen minutes is the standard time for the procedure (Figure 1).
-
Understand the thrombus dynamics.
-
Thrombus management should be a selective strategy that is based on thrombus grade for management of STEMI lesions.
-
STEMI intervention is a blind date. What a STEMI has in store can not be predicted.
-
D2B interventions are all about teamwork. There are 4 people who are involved in intervention; the patient, the ambulance emergency medical technician, the catheterization lab staff, and the cardiac interventionalist. It is possible to bypass a number of other road blocks to get the patient to the interventionalist as quickly as possible to reduce D2B time.
-
Predictable prehospital alert is the most definitive way of achieving recommended D2B times.
-
Integrated, population-based AMI programs are essential.
-
STEMI interventions demand a broad public health perspective. There are many people who are involved with the STEMI process, not just the interventional cardiologist.
-
Family Physician: Learn about current treatment options that exist for primary and secondary prevention of MI; Cardiologist: Initiate early treatment with antiplatelet agents; β-blockers, anti-coagulants; narcotics; fibrinolytics where appropriate; master triage and transfer
-
Interventional Cardiologist: Expert in short D2B STEMI interventions
-
Media: Educate patients, monitor results, and compliance
-
Hospital: Provide exceptional emergency department, laboratory, and cardiac care unit services
-
Patient: Take care of yourself; know of treatment options; seek treatment early
-
Politicians/Leaders: Allocate appropriate resources; the next patient may be you or your loved one
-

Procedure Timeline.
Reproduced with permission from S. Mehta, MD.
The Ten Commandments of STEMI.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.