

Summary
Rapid myocardial reperfusion is the primary goal in patients with ST-segment elevation myocardial infarction, and the extent to which early reperfusion is achieved is the main factor in determining the extent of the early and long-term clinical benefit of treatment. This article discusses several approaches to improving outcomes in these patients.
- interventional techniques & devices clinical trials
- myocardial infarction
Rapid myocardial reperfusion is the primary goal in patients with ST-segment elevation myocardial infarction (STEMI), and the extent to which early reperfusion is achieved is the main factor in determining the extent of the early and long-term clinical benefit of treatment. Rajesh M. Dave, MD, Ortenzio Heart Center, Harrisburg, Pennsylvania, USA, reviewed several approaches to improving outcomes in these patients.
Two methods for achieving reperfusion include percutaneous coronary intervention (PCI) and fibrinolysis. The success of PCI is frequently assessed in terms of ST-segment elevation resolution or return to normal angiographic TIMI (TIMI 3) flow. Dr. Dave suggested that these two measures may not go far enough. He cited myocardial blush grade (MBG), an angiographic measure of myocardial perfusion, which has been shown to be independently associated with mortality [Svilaas T et al. New Engl J Med 2008; Kampinga MA et al. Circ Cardiovasc Interv 2010], and suggested that MBG should be documented in addition to TIMI flow as a measure of PCI success.
Catheter-based thrombectomy is a newer modality that may improve reperfusion and outcomes in STEMI patients who are treated with urgent PCI. In a pooled analysis of data from more than 2500 patients in 11 clinical trials, Burzotta and colleagues showed that thrombectomy (in particular, manual thrombectomy) significantly improves the clinical outcome in patients with STEMI who are undergoing mechanical reperfusion and that its effect may be enhanced with the addition of potent antiplatelet therapy (eg, GP IIb/IIIa inhibitors) [Burzotta F et al Eur Heart J 2009].
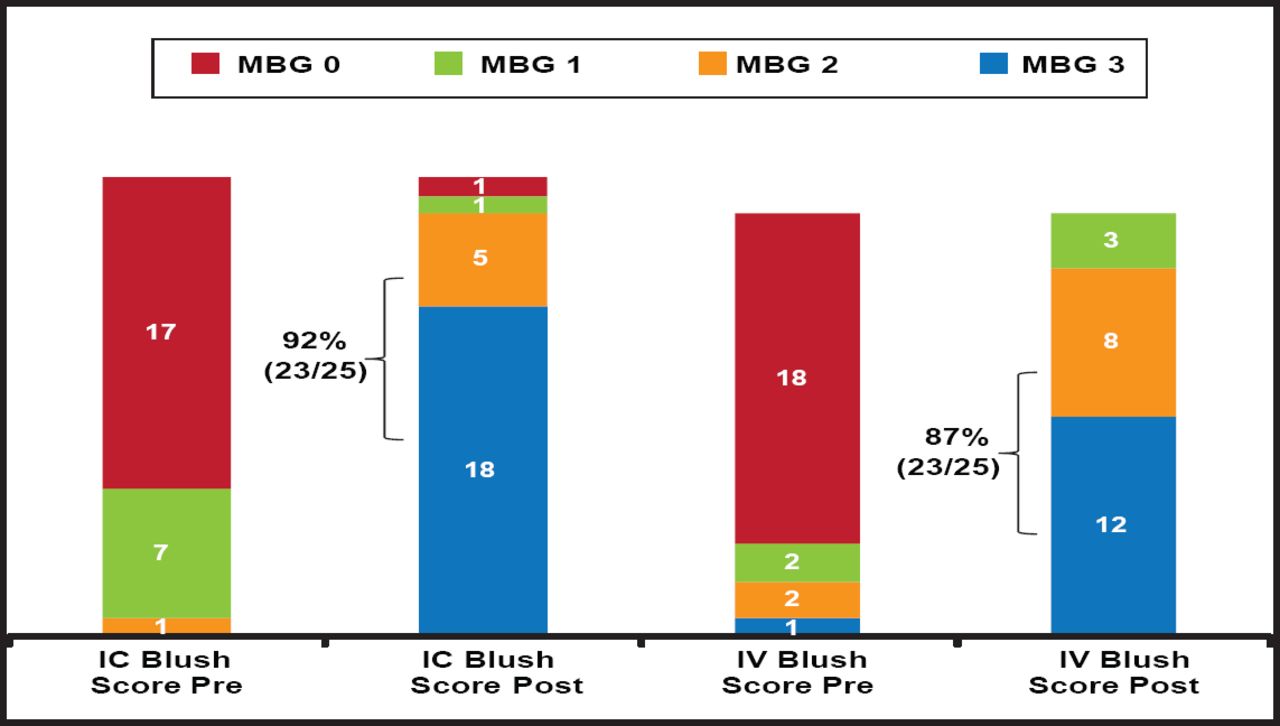
Dr. Dave discussed the results of CRYSTAL AMI, a single-center, prospective, randomized, proof-of-concept study of intravenous (IV) abciximab versus intracoronary (IC) abciximab in patients with acute myocardial infarction who were undergoing PCI within 6 hours of symptom onset. All patients received heparin and a 600-mg clopidogrel load. The use of thrombectomy devices was permitted. MBG, TIMI flow, and ST resolution were evaluated at the end of the procedure, and left ventricular function was evaluated by echocardiography at discharge. Echocardiography was repeated at 30 days, at which time patients also underwent a resting Sestamibi scan. In the IC group 92% of patients achieved the primary endpoint of postprocedure MBG >2 versus 86% of patients who received IV therapy (Figure 1). TIMI flow was also higher among patients who received IC therapy (96%) versus those who received IV therapy (82%). There were no readmissions or deaths in the IC arm versus 2 readmissions and 1 death among patients who received IV therapy. There were no major bleeds in either group.

MGB Score.
Reproduced with permission from R. Dave, MD.
“Improving myocardial preservation in patients presenting with STEMI has profound economic impact through reduced cost of care, improved quality of life, and less need for ICD implantation.” This approach is being further evaluated in the INFUSE-AMI study, a randomized, multicenter, single-blind evaluation of IC abciximab infusion and aspiration thrombectomy in patients who are undergoing PCI for anterior STEMI that is currently recruiting [Gibson CM et al. Am Heart J 2011; NCT00976521].
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.