

Summary
The HEart function Assessment Registry Trial in Saudi Arabia [HEARTS] is a nationwide medical registry of heart failure (HF) throughout Saudi Arabia. The goal of the registry is to study practice patterns in the management of patients with acute HF to assess the gap between practice and evidence, to improve the quality of cardiac care that is provided, and to establish heart function clinics across the country that will reduce the morbidity and mortality of HF disease by appropriately managing high-risk chronic HF patients.
- cardiology clinical trials
- heart failure
The HEart function Assessment Registry Trial in Saudi Arabia (HEARTS) is a nationwide medical registry of heart failure (HF) throughout Saudi Arabia. The goal of the registry is to study practice patterns in the management of patients with acute HF to assess the gap between practice and evidence, to improve the quality of cardiac care that is provided, and to establish heart function clinics across the country that will reduce the morbidity and mortality of HF disease by appropriately managing high-risk chronic HF patients.
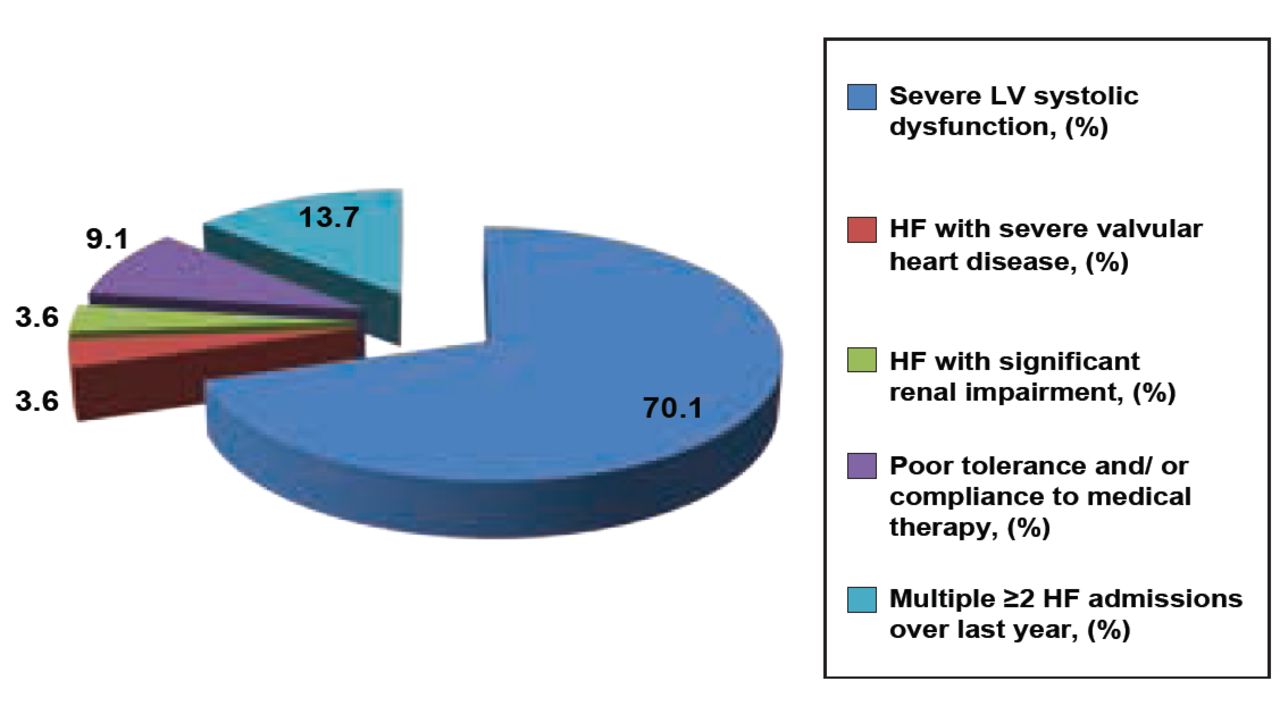
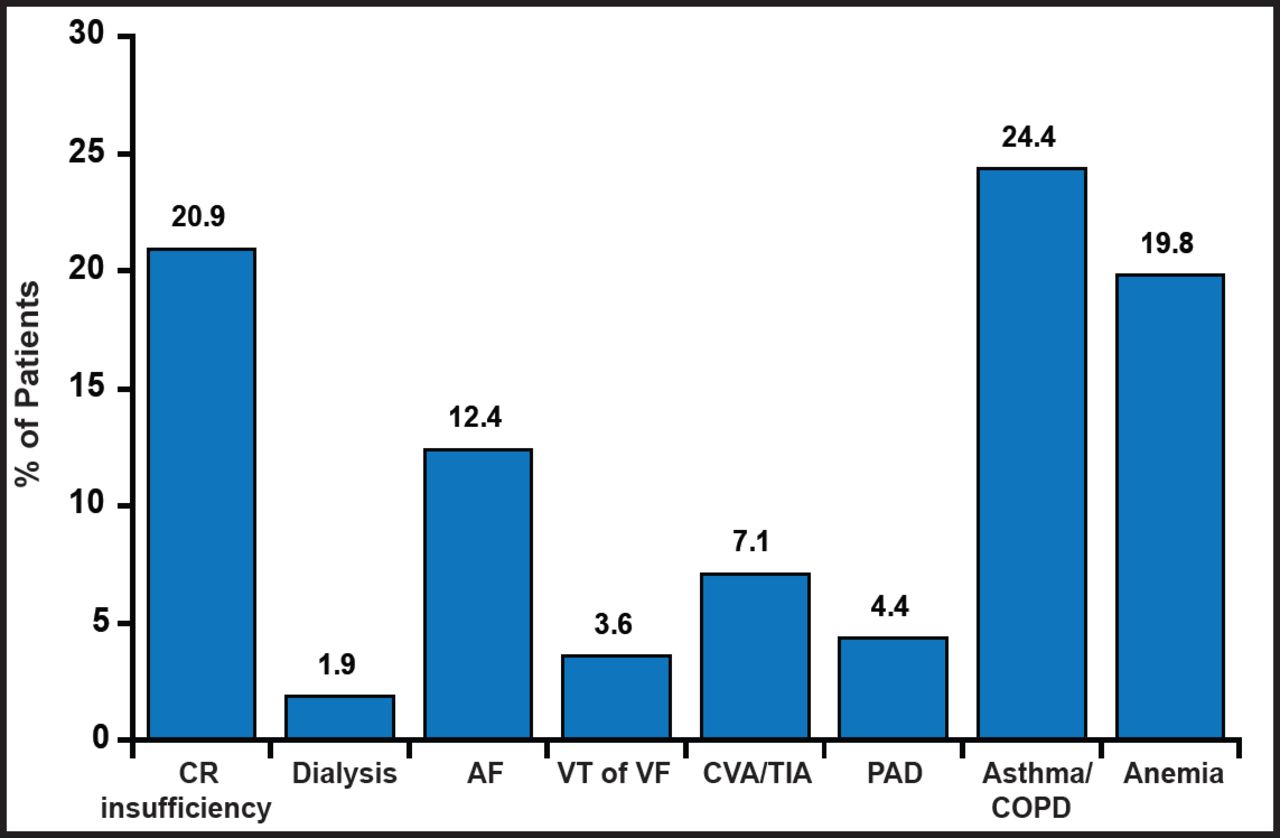
Abdelfatah Elasfar, MD, King Fahad Medical City, Riyadh, Saudi Arabia, presented the preliminary results for 368 patients from two tertiary care hospitals in Saudi Arabia with established multidisciplinary HF centers. The majority of patients (73.4%) was referred to the HF center by a cardiologist, 9.6% by the emergency department, and 17% by other services. The most common reason for referral was severe left ventricular (LV) dysfunction (70.1%). Other reasons are shown in Figure 1. Almost 50% of patients who were referred to the clinic were aged between 50 and 70 years; however, 34% was >50 years. Most patients were men (71.3%); almost all were Saudi (>95%). The most common traditional risk factor among patients who were referred to the clinic was hypertension (74.7%), followed by ischemic heart disease (41.8%). More than 21% of patients were smokers, 53% had diabetes mellitus, and 57% had dyslipidemia. Associated comorbidities are shown in Figure 2. Implantable cardioverter defibrillators (ICDs) were present in 28.8% of patients and cardiac resynchronization devices were in 8%. Most patients were New York Heart Association (NYHA) class II (36.3%) or III (49.5%). One-half of all patients reported fatigue, one-third peripheral edema, and ∼28% orthopnea/paroxysmal nocturnal dyspnea. Only 5.2% reported palpitations. Median (IRQ) sitting systolic blood pressure was 119 mm Hg (range 73 to 213). Median heart rate was 77 beats per minute (range 52 to 154). LV dysfunction was severe in 75.3% of patients.

Reasons for Referral.
Reproduced with permission from A. Elasfar, MD.

Associated Comorbidities.
CR=cardio renal; AF=atrial fibrillation; VT=ventricular tachycardia; VF=ventricular fibrillation; CVA=cerebral vascular accident; TIA=transient ischemic attack; PAD=pulmonary artery disease; COPD=chronic obstructive pulmonary disease.
Reproduced with permission from A. Elasfar, MD.
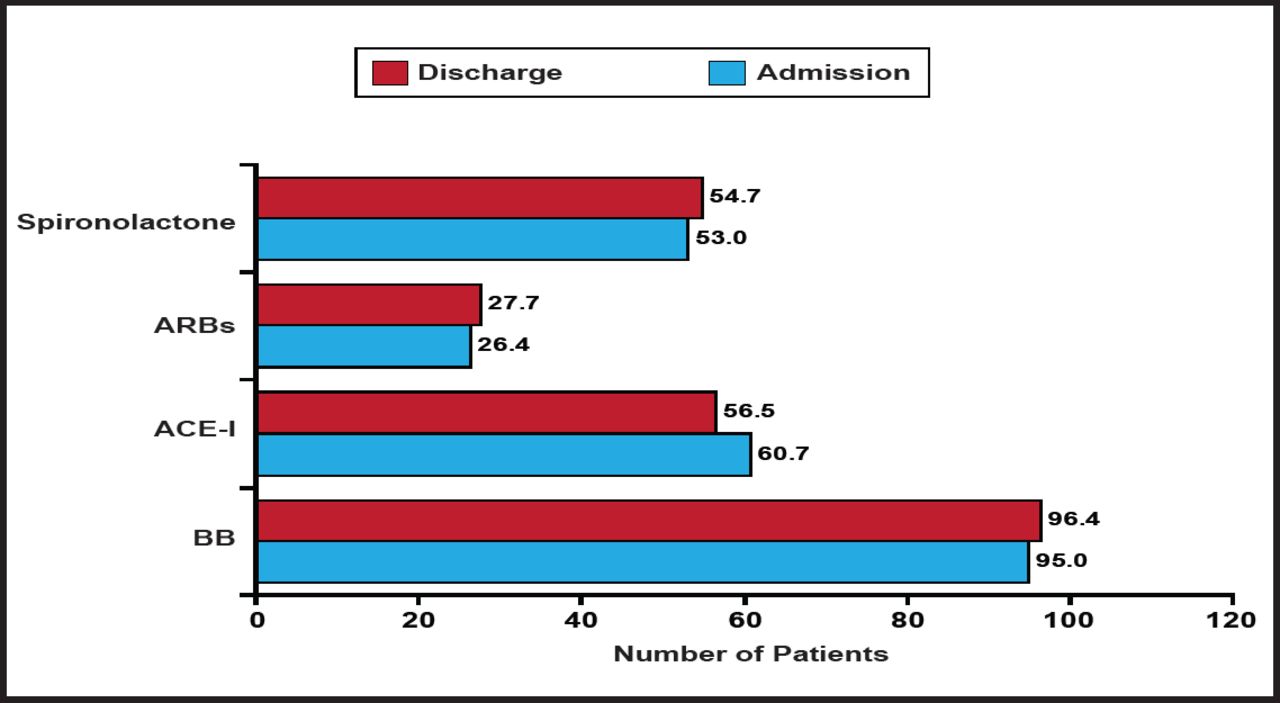
Almost 90% of patients were receiving furosemide, 83% aspirin, 74% statins, 40% digoxin, and 38% nitrates. Most patients were prescribed one or more specific HF medications at admission and at discharge (Figure 3). HF was described as nonischemic dilated cardiomyopathy in 45.6% of patients and ischemic in 38.2% of patients. Only 8.2% of patients were described as having hypertensive heart disease. Of the 368 patients who were referred to the HF clinic, 88% is still alive and 3% has died; 9% has been lost to follow-up.

Specific HF Medications.
Reproduced with permission from A. Elasfar, MD.
Compared with HF patients in developed countries, outpatients with high-risk HF in Saudi Arabia are younger, have much higher prevalence of diabetes mellitus and hypertension, and predominantly have LV systolic dysfunction. The rate of evidence-based therapy use was reasonable, but the ICD/cardiac resynchronization therapy implantation rate was low.
The study is limited by its small sample size, its location in only tertiary care hospitals, and limited geographic representation. Further improvements in management and potential clinical outcomes are yet to be shown with long-term follow-up at the HFC
Additional information about HEARTS is available at: www.hearts-ksa.com/home.html.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.