

Summary
Gender-specific differences in cardiovascular medical treatment are not entirely unexpected, due to gender differences in physiology and pharmacodynamics, symptomology, treatment response, and representation in clinical trials.
- Hypertensive Disease
- Heart Failure
- Lipid Disorders
Gender-specific differences in cardiovascular (CV) medical treatment are not entirely unexpected, due to gender differences in physiology and pharmacodynamics, symptomology, treatment response, and representation in clinical trials. Ernst Van der Wall, MD, PhD, Leiden University Medical Center, Leiden, the Netherlands, discussed these differences.
Cardiovascular disease (CVD) is the primary cause of death among women, killing 8.6 million women worldwide every year. Yet, a significant gender gap exists in treatments that are offered to women compared with men. For example, the time from symptom onset to hospital presentation for myocardial infarction (MI) is greater in women (3.46% longer time to presentation; 95% CI, 1.06 to 5.92; p=0.005), despite national campaigns that are aimed at increasing women's awareness of their risk of heart disease [Dierks DB et al. Am Heart J 2010].
Historically, randomized clinical trials have included a majority of men, although this has changed over time. A systematic review of treatment of mild to moderate hypertension [Ljungman C et al. J Womens Health 2009] showed an increase in the proportion of women with hypertension (r=0.27; p<0.05). Another study found that all treatments that were studied provided broadly similar protection against major CV events in men and women (p-homogeneity >0.08) [Turnbull F et al. Eur Heart J 2008].
A meta-analysis on statin therapy in the two sexes found that statin therapy reduced the risk of coronary heart disease events in men without prior CVD but not in women. No differences between the genders were found regarding total mortality [Petretta M et al. Int J Cardiol 2010]. Another study showed that women might be less responsive to aspirin than men in preventing nonfatal MI. Trials predominantly with female subjects indicated a much lower risk reduction than those that were made up mostly of men (RR, 0.87 [95% CI, 0.71 to 1.06] vs RR, 0.62 [95% CI; 0.54 to 0.71]) [Yerman T et al. BMC Med 2007].
Evidence-based guidelines for CVD prevention in women have been revised on the basis of more definitive data about menopause, aspirin, and folic acid therapies. Class III interventions that are not useful/effective and may be harmful for CVD or MI prevention in women have been specified. Hormone therapy and selective estrogen receptor modulators, antioxidant vitamin supplements (vitamins E, C, and beta-carotene), and folic acid should not be used for primary or secondary prevention of CVD [Mosca L et al. Circulation 2007].
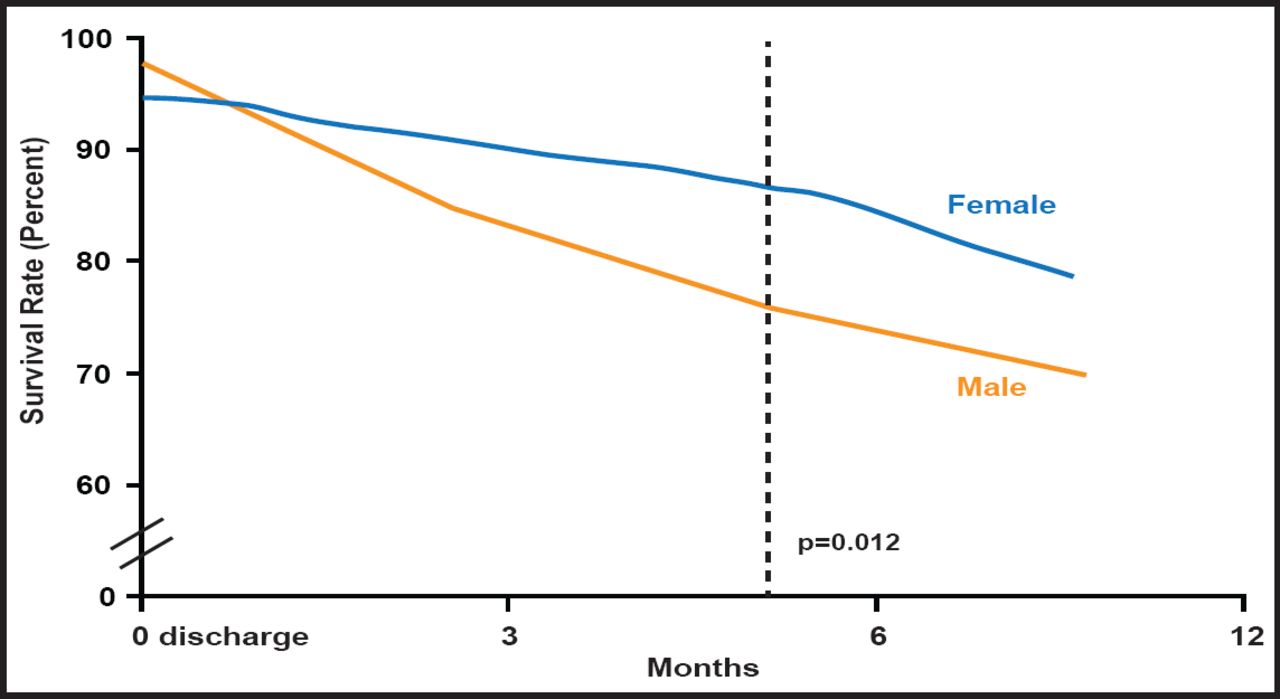
Prof. van der Wall pointed out that there may be differences in the underlying causes of and outcomes that are related to heart failure in women compared with men. For example, women who are admitted to the hospital with heart failure have better 1-year survival rates than their male peers (Figure 1) [Mejhert M et al. Eur J Heart Failure 1999]. In addition, testosterone treatment may not benefit men with heart failure but may benefit women [van der Wall EE. Neth Heart J 2011]. Of note, 30-day mortality after PCI in men and women has decreased in the past 25 years, with no differences in short- or long-term mortality between men and women [Prasad A et al. JACC 2008].

Survival Rates with Respect to Gender in Patients Admitted with Heart Failure 1 Year After Hospital Discharge.
Reproduced with permission from Oxford University Press. Diagnostic tests, treatment and follow-up in heart failure patients — is there a gender bias in the coherence to guidelines? Mejhert M et al. Eur J Heart Fail. Dec 17, 1999.
Many women are unaware of specific risk factors and assume they are less likely to suffer from stroke, heart failure, or heart attack. But, this assumption is incorrect. Prof. van der Wall noted that prescribing physicians should be aware of gender-specific treatments, that all guidelines should account for gender-specific differences, and that such guidelines should be implemented accordingly.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.