

Summary
Steroids have an important place in the treatment of bacterial meningitis.
- Bacterial Infections
- Inflammatory Diseases
Steroids have an important place in the treatment of bacterial meningitis (BM), according to W. Michael Scheld, MD, University of Virginia, Charlottesville, Virginia, USA. Dr. Scheld was unable to attend this year's ICAAC, but graciously agreed to share highlights from that talk for the benefit of MD Conference Express readers.
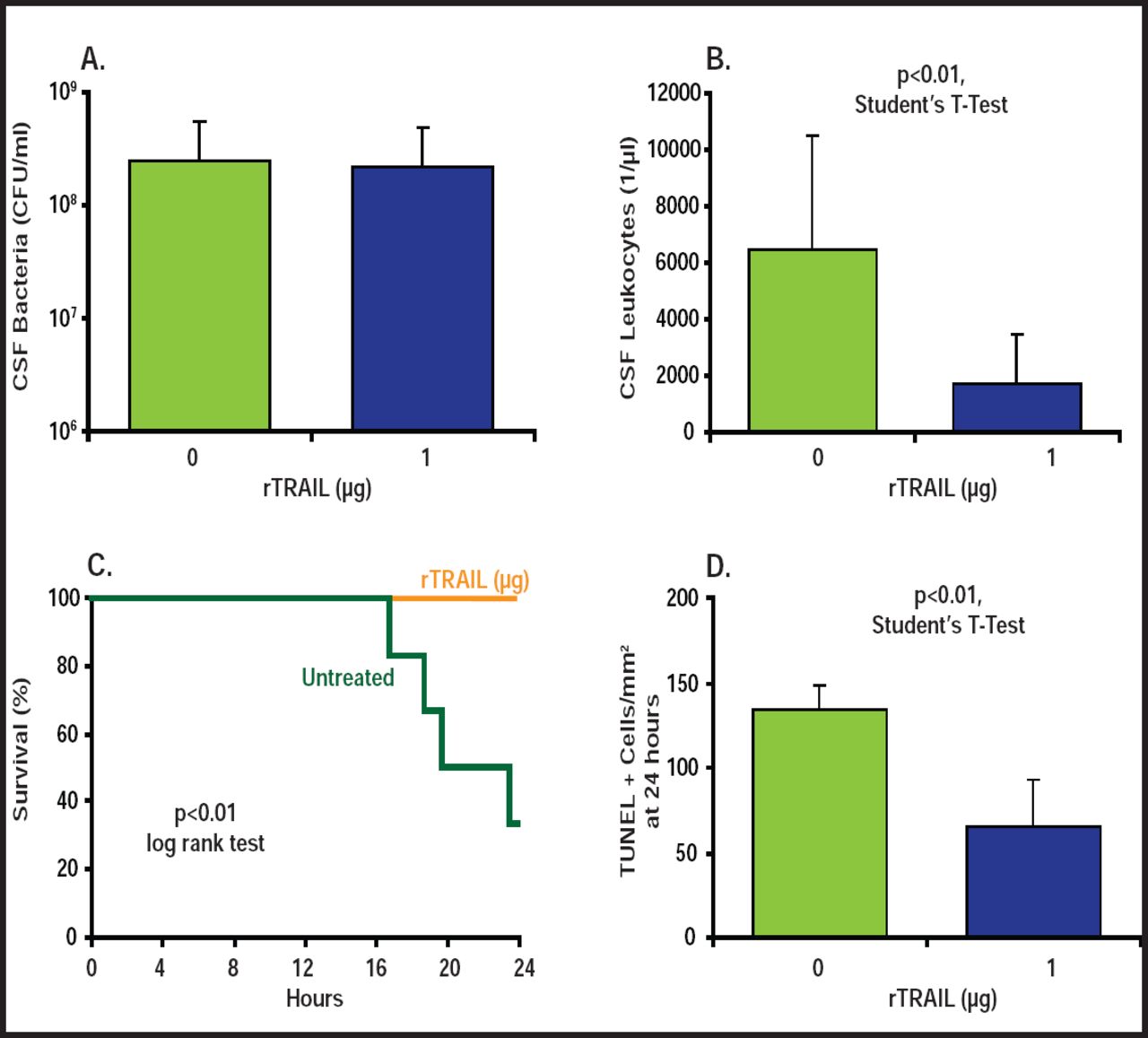
The rationale for employing anti-inflammatory medication in the treatment of BM is based upon the observation that hyperactive central nervous system (CNS) immune responses underlie brain swelling and neuronal loss and likely contribute to morbidity and mortality. In animals, steroids have been shown to reduce CNS inflammation, intracranial pressure, and neuronal loss. In addition, new investigational anti-inflammatory agents, such as recombinant tumor necrosis factor-related apoptosis-inducing ligand (rTRAIL), significantly decrease cerebrospinal fluid leukocytes and apoptosis in mouse models of pneumococcal meningitis and significantly improve survival (Figure 1) [Hoffmann O et al. J Clin Invest 2007].

Effects of Treatment with rTRAIL in Meningitis Induced By Live pneumococci in Mice.
(A) At 24 hours after infection, CSF bacterial load in untreated and rTRAIL-treated wild-type mice did not differ. (B) CSF leukocyte concentration was significantly lower in rTRAIL-treated mice than in controls. **p<0.01, Student's t-test. (C) Mortality was higher in untreated versus rTRAIL-treated mice. **p<0.01, log rank test. (D) Apoptosis was reduced by treatment with rTRAIL. **p<0.01, Student's t-test.
After review of the clinical literature over the past decade, Dr. Scheld believes that intravenous dexamethasone for the first 2 to 4 days in the treatment of community-acquired BM is indicatedin all ages in developed nations. De Gans et al. demonstrated an overall reduced risk for unfavorable outcomes and mortality in adults (RR=0.59; 95% CI, 0.37 to 0.94; p=0.03; and RR=0.48; 95% CI, 0.24 to 0.96; p=0.04, respectively) with dexamethasone [New Engl J Med 2002]. Data from the Netherlands reveal that national implementation of adjunctive dexamethasone in patients with S. pneumoniae BM has significantly reduced unfavorable outcomes, hearing loss, and mortality [Brouwer MC et al. Neurology 2010].
In contrast, steroids are not recommended where resources are limited and in populations with high HIV-positivity rates. A Vietnamese study showed a benefit to dexamethasone use only among patients with a proven microbiological diagnosis of BM but not among those with a probable diagnosis [Nguyen TH et al. New Engl J Med 2007]. A study in Malawi among patients with high rates of HIV infection showed no benefit to using steroids in the treatment of BM [Scarborough M et al. New Engl J Med 2007]. Further, a 2010 meta-analysis that examined the issue showed that benefits of reduced hearing loss and neurologic sequelae, but not overall mortality among patients with BM who were treated with adjunctive steroids were observed in developed nations only [Brouwer MC et al. Cochrane Rev 2010].
Other potential strategies for improving BM outcomes include selection of highly bactericidal, non lytic antibacterials such as rifampin, which has been shown to reduce β-lactam-induced cytotoxicity in animals [Spreer A et al. Crit Care Med 2009], and daptomycin plus ceftriaxone, which has been associated with reduced neuronal injury and hearing loss [Grandgirad et al. ECCMID 2009]. In addition, prompt initiation of antibacterial therapy has been shown to reduce mortality [Proulx N et al. Q J Med 2005; Auburtin M et al. Crit Care Med 2006] and remains a central tenant of proper treatment.
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.