

Summary
While the Penumbra Pivotal Stroke Trial demonstrated a recanalization rate of 81.6%, the rate of good clinical outcome, defined as a modified Rankin Scale (mRS) score =2, was relatively low (25%) [The Penumbra Pivotal Stroke Investigators. Stroke 2009]. This article discusses a subanalysis from the Penumbra Pivotal Stroke Trial, which evaluated whether a good initial noncontrast computed tomography and short time to recanalization predicted good clinical outcome in patients with acute ischemic stroke who were undergoing endovascular procedures.
- neurology
- neurology clinical trials
- interventional techniques & devices
- neuroimaging
- cerebrovascular disease
While the Penumbra Pivotal Stroke Trial demonstrated a recanalization rate of 81.6%, the rate of good clinical outcome, defined as a modified Rankin Scale (mRS) score ≤2, was relatively low (25%) [The Penumbra Pivotal Stroke Investigators. Stroke 2009]. Mayank Goyal, MD, University of Calgary, Calgary, Alberta, Canada, presented a subanalysis from the Penumbra Pivotal Stroke Trial.
The aim of this substudy was to evaluate whether a good initial noncontrast computed tomography (NCCT), defined as >7 according to the ASPECTS scoring system, and short time to recanalization predicted good clinical outcome in patients with acute ischemic stroke who were undergoing endovascular procedures. The substudy included 85 of the original 125 Penumbra trial participants (median age 64.1 years), stratified by blinded NCCT reading at presentation. Patients were grouped according to NCCT ASPECTS score of >7 or ≤7 (median ASPECTS score at baseline was 6). ASPECTS scores were categorized as good (8 to 10; observed in 36.5% of patients), intermediate (5 to 7), and poor (0 to 4). The primary outcome was mRS ≤2 at 3 months.
Medical comorbidities at baseline included hypertension (n=83), diabetes (n=23), and atrial fibrillation (n=34). Occlusions were located in the internal carotid artery in 22.4% of patients (19.3% had ASPECTS scores >7 vs 24.1% ≤7), in the M1 main coronary artery in 63.5% of patients (61.3% had ASPECTS scores >7 vs 64.8% ≤7), and in the M2 main carotid artery in 14.1% of patients (19.3% had ASPECTS scores >7 vs 11.1% ≤7) at baseline.
TIMI scores of 2 to 3 were noted in 81.2% of patients. Of the patients with ASPECTS scores >7, 83.9% had TIMI 2 to 3 recanalization compared with 79.6% with ASPECTS scores ≤7 (p= 0.8). At 3 months, mRS 0 to 2 was observed in 27.1% of patients, 50% in the ASPECTS scores >7 group, and 15% in the ASPECTS scores ≤ 7 group (Table 1). When broken down by ASPECTS categories of good, intermediate, and poor, good clinical outcome was significantly greater in the >7 group compared with the ≤7 group (RR 3.3; 95% CI, 1.6 to 6.8; Table 1), and no patient with an ASPECTS score ≤4 (poor scan, n=28) had good clinical outcome. Additionally, good clinical outcome was significantly higher in the early recanalizer (≤300 minutes) group compared with the combined late recanalizer (>300 minutes) or nonrecanalizer (TIMI 0 to 1) group (RR 2.3; 95% CI, 1.2 to 4.4). No patient without recanalization (TIMI 0 to 1; n=16) did well.
Clinical Outcomes Stratified by Baseline CT ASPECTS Score.
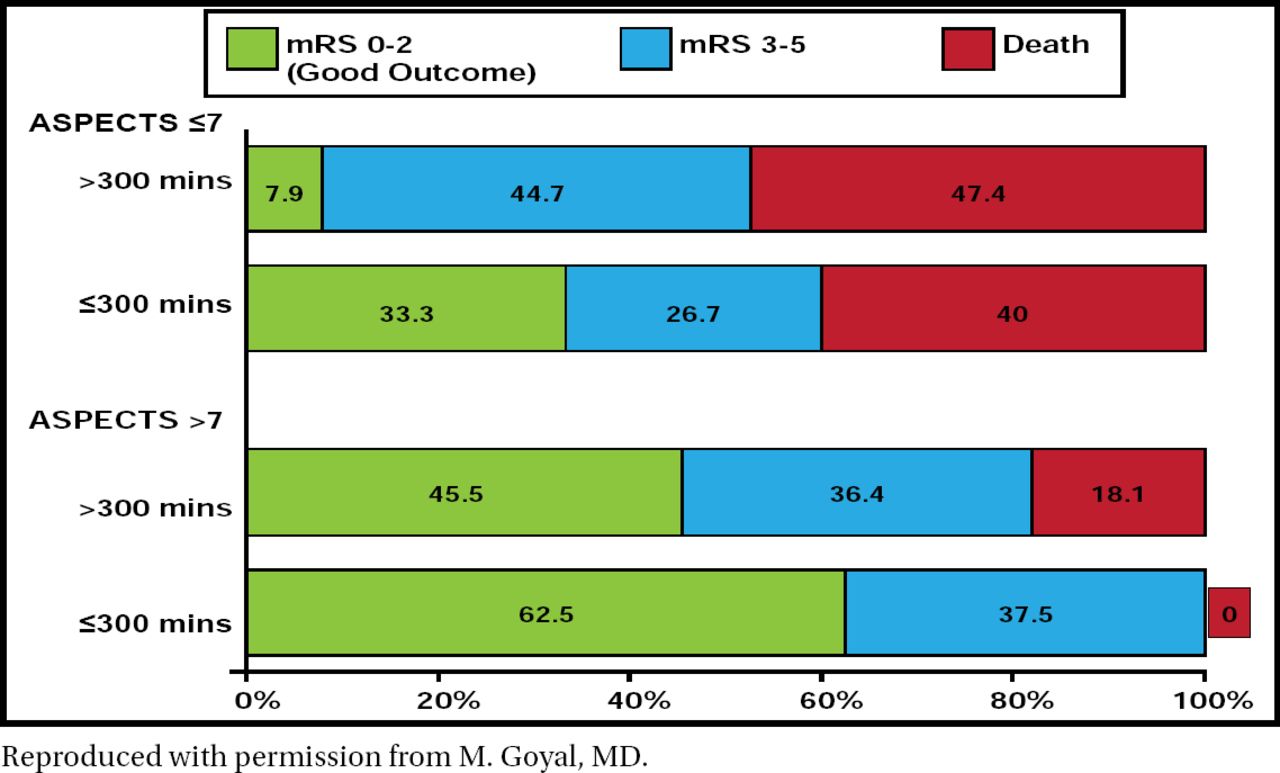
After adjusting for baseline stroke severity, there was evidence of an ASPECTS score and onset-to-recanalization time interaction. The direction of interaction was such that among patients with ASPECTS scores >7, the relative effect of onset-to-recanalization time (≤300 minutes or >300 minutes) in predicting outcome was small. Among patients with ASPECTS scores ≤7, only those with an onset-to-recanalization time ≤ 300 minutes had some chance of achieving a functional outcome (Figure 1).

Clinical Outcome (mRS at 3 months) in Two Groups, ASPECTS Scores >7 and ≤7, Stratified By Onset-to-Recanalization Time <300 Minutes and ≥300 Minutes.
Reproduced with permission from M. Goyal, MD.
Dr. Goyal concluded that faster recanalization and proper patient selection that is based on initial NCCT contribute to the achievement of good clinical outcomes in patients with acute ischemic stroke who undergo endovascular procedures.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.