

Summary
The benefits of antihypertensive drugs vary by therapeutic strategy, and the search continues for optimal treatment. While guidelines have been developed to manage hypertension (HT), research continues to emerge that occasionally conflicts with current recommendations. Despite progress being made in the area of HT research, many questions remain unanswered. This article discusses recent data from clinical trials and how they pertain to current hypertensive treatment strategies, as well as trial needs moving forward.
- Hypertensive Disease
Medical therapy for the treatment of hypertension (HT) began about 50 years ago. The benefits of antihypertensive drugs vary by therapeutic strategy, and the search continues for optimal treatment. While guidelines have been developed to manage HT, research continues to emerge that occasionally conflicts with current recommendations. Despite progress being made in the area of HT research, many questions remain unanswered. Alberto Zanchetti, MD, Istituto Auxologico Italiano, Università di Milano, Milan, Italy, discussed recent data from clinical trials and how they pertain to current hypertensive treatment strategies, as well as trial needs moving forward.
According to 2007 ESH-ESC guidelines, the use of antihypertensive treatment (ie, thiazide diuretics, β-blockers, calcium antagonists, ACE inhibitors, and angiotensin receptor antagonists) to lower blood pressure (BP) can be beneficial for patients with varying degrees of HT. However, each of the recommended classes may be associated with specific advantages and limitations that should be considered when choosing an appropriate therapeutic regimen [2007 ESH-ESC Guidelines on Hypertension. J Hypertens 2007]. The issue of whether or not BP lowering is beneficial in all hypertensives remains unclear and may be dependent upon hypertensive grade, risk stratification, and patient demographics (eg, age). There has also been some debate as to what the optimal BP target should be and whether or not lower is, in fact, better.
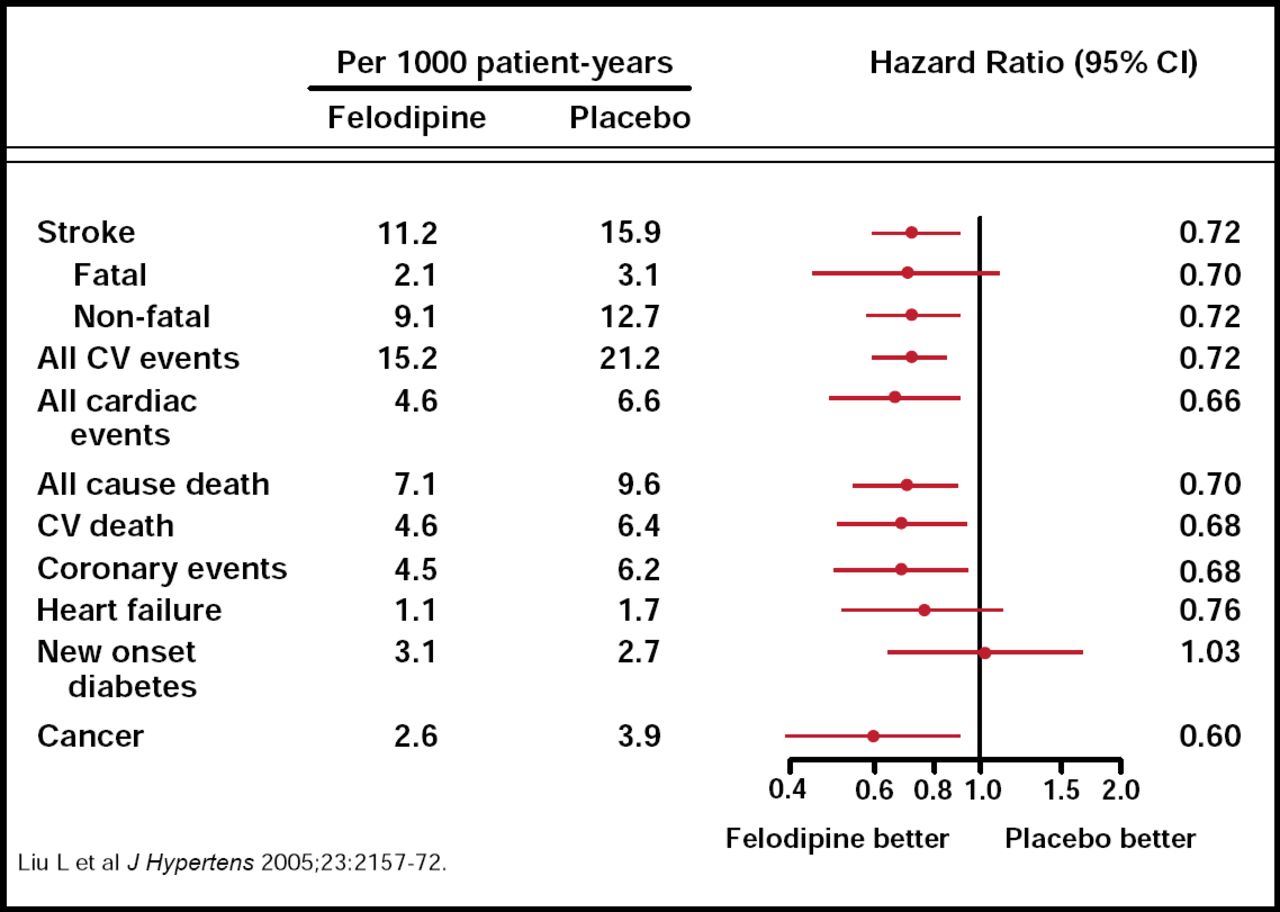
In the large, double-blind, randomized, placebo-controlled Felodipine Event Reduction (FEVER) study, evaluating the effect of combination low-dose diuretic and low-dose calcium antagonist (versus low-dose diuretic monotherapy) on the incidence of stroke and other cardiovascular events, small differences in BP (a little as 4/2 mm Hg systolic BP/diastolic BP [SBP/DBP]) were associated with substantial reductions in the incidence of cardiovascular events. FEVER included 9800 Chinese patients (mean age 61.5 years) with hypertension and one or two additional cardiovascular risk factors (range 140–180 mm Hg SBP/90–100 mm Hg DBP 6 weeks after switching from previous antihypertensive therapy to low-dose hydrochlorothiazide [HCTZ]). Patients were randomized to receive either low-dose felodipine extended-release or placebo.
Mean BP from randomization to last follow-up went from 154.2/91.0 mm Hg to 137.3/82.5 mm Hg in the felodipine group (vs 154.4/91.3 mm Hg to 142.5/85.0 mm Hg in the placebo group). The primary endpoint of fatal and nonfatal stroke was reduced by 27% in the felodipine group compared with placebo (p=0.001). The felodipine group also demonstrated reductions in all cardiovascular events (27%), all cardiac events (35%), death by any cause (31%), coronary events (32%), heart failure (30%), cardiovascular death (33%), and cancer (36%; Figure 1).

Endpoint Analysis (First-Time Occurrence in Each Category).
Reproduced with permission from
The SBP that was achieved in FEVER was slightly below the recommended goal of <140 mm Hg, while those in the placebo group remained >140 mm Hg, suggesting a protective effect of lower SBP that extended to those at moderate risk or grade 1 (stage 1) hypertension [Liu L et al. J Hypertens 2005]. Prof. Zanchetti pointed out, however, that 35% of FEVER patients had SBP ≥160 mm Hg after switching to HCTZ (grade 2 hypertension). Though lower SBP goals for the elderly may also be implied, based on these and other trial analyses, Prof. Zanchetti cautions that solid evidence is needed before treatment strategies in this cohort can be modified. To date, trial evidence that supports SBP <140 mm Hg in the elderly is missing [Zanchetti A et al. J Hypertens 2009].
Further analysis of FEVER revealed a number of additional risk factors that increased residual risk despite effective antihypertensive treatment. Higher baseline SBP and smoking conferred an increase in cardiovascular events and stroke risk. Other factors, such as male gender, older age, diabetes, and prior cardiovascular disease, were also associated with higher incidence of cardiovascular events. Isolated systolic HT, left ventricular hypertrophy, and high serum cholesterol did not appear to impact cardiovascular risk markedly [Zhang Y et al. J Hypertens 2010]. Additional subanalysis data from the FEVER study are still pending.
While the FEVER trial provided valuable data about BP lowering in patients at moderate risk, there is still uncertainty about the extent to which BP should be lowered and the J-curve dilemma, which is the point beyond which blood pressure reduction in patients with HT becomes deleterious rather than beneficial, particularly related to cardiovascular outcomes.
A reappraisal of European guidelines on HT management addressed the issue of the J-curve in 2009. This recommendation acknowledged the existence of a J-curve in principle (at 0 mm Hg all individuals are dead) but stated that in individuals without cardiovascular disease, the BP-cardiovascular event relationship is linear to very low (∼110/70 mm Hg) BP values. However, high-risk patients may experience a higher threshold (J-curve) due to impaired mechanisms that are related to blood flow autoregulation [Mancia G et al. J Hypertens 2009].
Evidence from trials that have investigated the J-curve directly is unfortunately very sparse. Results from the Hypertension Optimal Treatment (HOT) study in the late 1990s refuted the existence of the J-curve [Hansson L et al. Lancet 1998]. However, this may be related to the timing and design of the study. This study was designed at a time when interest was focused primarily on DBP measurements, and SBP was reduced less aggressively. Furthermore, the HOT study population included lower-risk patients, which may have influenced results.
In the recent ACCORD-BP study, intensive BP control (target SBP<120 mm Hg) did not reduce the rate of major cardiovascular events compared with standard BP control (SBP<140 mm Hg) in patients with type 2 diabetes mellitus [The ACCORD Study Group. N Engl J Med 2010]. It is important to note that this study was limited to only two study arms, and there was a large difference in SBP between the two study arms (133.5 mm Hg vs 119.3 mm Hg). Also, the incidence of cardiovascular events was only half of what was expected (2% rather than 4% per year). Therefore, Prof. Zanchetti explained that it can not be excluded that lower SBP target is accompanied by some benefit or that there is an intermediate SBP level (between 134 mm Hg and 119 mm Hg) at which benefits are greater than at 134 mm Hg and 119 mm Hg (J-curve).
Based on the lack of direct evidence on the J-curve, an indirect approach has been used, which plots incidence of outcomes against achieved BP in randomized trials. There are many limitations in this approach. It necessarily relies upon post hoc analyses. At the extremes of the curves, there are only a small number of individuals with a very small number of events, and different patient risk characteristics require statistical adjustments with consequent uncertainties. Additionally, different studies have shown different nadir BP values (the values below which risk starts to increase), which makes it difficult to evaluate the veracity of a J-curve. Randomization is also lost during post hoc analysis, which poses a further challenge for evaluation.
It must be acknowledged that there are still gaps in evidence that is related to the optimum BP goal to be achieved in order to maximize cardiovascular risk reduction. New randomized trials are needed to provide data regarding the benefits and limits of aggressive BP lowering. More data about specific management strategies for particular groups of hypertensive patients (ie, according to risk stratification, age, HT grade, and previous stroke or myocardial infarction) are also warranted. While we are getting closer to finding optimal BP goals, as demonstrated by modified guidelines and emerging evidence, new trials are required to ensure that the appropriate therapeutic approaches are being utilized in clinical practice.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.