

Summary
Each year, during its annual congress, the ESC introduces new and/or updated Clinical Practice Guidelines that represent the most current evidence-based medicine. The following are selected recommendations from four Practice Guidelines that were presented this year including: updates to the 2008 ESC guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure and the 2007 ESC guidelines for Cardiac and Resynchronization Therapy. Two expanded Class Ia recommendations were also released.
- Arrhythmias
- Coronary Artery Disease
- Heart Failure
- Interventional Techniques & Devices
- Cardiology Guidelines
Each year, during its annual congress, the ESC introduces new and/or updated Clinical Practice Guidelines that represent the most current evidence-based medicine. The following are selected recommendations from four Practice Guidelines that were presented this year.
Kenneth Dickstein, MD, University of Bergen, Stavanger, Norway, presented updates to the 2008 ESC guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure and the 2007 ESC guidelines for Cardiac and Resynchronization Therapy (CRT), which were developed in collaboration with the Heart Failure Association and the European Heart Rhythm Association (EHRA). Two expanded Class Ia recommendations were released:
-
CRT-P/CRT-D is recommended to reduce morbidity and mortality in NYHA class III/IV patients with LVEF of ≤35% and QRS width of ≥120 ms with a conventional indication for an ICD. This recommendation is supported by the COMPANION [Bristow MR et al. N Engl J Med 2004] and CARE-HF [Cleland JG et al. N Engl J Med 2005] trials. Similar levels of evidence support CRT-P.
-
CRT, preferentially by CRT-D, is recommended to reduce morbidity or to prevent disease progression in NYHA class II patients, LVEF≤35%, QRS≥150 ms, and SR optimal medical therapy. The recommendations are supported by data from the MADIT-CRT [Moss AJ et al. N Engl J Med 2009] and REVERSE trials [Linde C et al. J Am Coll Cardiol 2008; Daubert C et al. J Am Coll Cardiol 2009].
Risk assessment and an appropriate choice of therapy are central to good clinical practice. The updated Joint ESC-EACTS Guidelines on Myocardial Revascularization, presented by Phillippe Kolh, MD, PhD, University Hospital of Liège, Liège, Belgium, and William Wijns, MD, FESC, Co-Director, Cardiovascular Centre, O.L.V.Z., Aalst, Belgium, include new guidance in both areas.
Patients who take an active role throughout the decision-making process have better outcomes. However, most patients who undergo CABG or PCI have limited understanding of their disease and its treatment. The new Guidelines recommend that patients be adequately informed about the potential benefits and short- and long-term risks of a revascularization procedure. Sufficient time for informed decision-making should be allowed. A sample patient information document is available in the Appendix in the online version of the Guidelines.
To facilitate an appropriate choice of therapy and help ensure the best patient outcome, the new Guidelines recommend multidisciplinary decision-making by a consolidated Heart Team in each institution. Collaboration and discussion between the clinical noninterventional cardiologist, the interventional cardiologist, and the cardiac surgeon are strongly recommended, as is the inclusion of other medical specialists (ie, nephrologists, diabetologists, neurologists, geriatricians), when treating patients with complex CAD and/or multiple associated comorbidities. The presenters emphasized the guideline recommendation that Heart Team members come to a patient strategy consensus prior to revascularization to maximize outcomes.
PCI presents an ideal example of the need for Heart Team/institutional agreement of strategic criteria. Ad hoc PCI (an interventional procedure that is performed while the patient is still on the catheterization table) may be well suited for some, but not all, patients. Although it can be cost-effective and associated with fewer access site complications, it is not appropriate for all patients and should not automatically be used as a default approach. Heart Teams and their institutions may want to consider PCI in a different session for patients with special considerations (Table 1).
Potential Indications for ad hoc PCI Versus Revascularization at an Interval.
The Guidelines also include recommendations on risk stratification scores to be used in candidates for PCI or CABG (Table 2):
Recommended Risk Stratification Scores in Candidates for PCI or CABG.
-
For PCI, the SYNTAX score is preferred to quantify the complexity of CAD
-
For CABG, both the EuroSCORE and STS score are well validated and predominantly based on clinical variables; however, the STS score undergoes periodic adjustments, which makes longitudinal comparisons difficult
New guidelines were issued concerning the indications for revascularization in stable angina or silent ischemia. The two issues that are addressed are: 1) the appropriateness of revascularization and 2) the relative merits of CABG and PCI in differing patterns of CAD. Current best evidence shows that revascularization can be readily justified:
-
On symptomatic grounds in patients with persistent limiting symptoms (angina or angina equivalent) despite optimal medical therapy, and/or
-
On prognostic grounds in certain anatomical patterns of disease AND a proven significant ischemic territory (even in asymptomatic patients). Significant left main stenosis and significant proximal left anterior descending disease, especially in the presence of multivessel CAD, are strong indications for revascularization. In the most severe patterns of CAD, CABG appears to offer a survival advantage as well as a marked reduction in the need for repeat revascularization, albeit at a higher risk of CVA, especially in left main disease.
Unlike many of the Guidelines, for which the majority of the recommendations is based on level A or B evidence, those for Grown-up Congenital Heart Disease (GUCH) rely mainly on Level C and some Level B evidence, due to the limited number of randomized clinical trials and the very few large nonrandomized trials in this relatively young specialty. Helmut Baumgartner, MD, University Hospital Muenster, Muenster, Germany, presented the new Guidelines.
Important changes include more precise definitions and guidance concerning:
-
Indications for cardiac magnetic resonance (CMR) and cardiac catherization; eg, CMR as an alternative to echo when both techniques can provide similar information but when echo can not be obtained with sufficient quality, and specific recommendations for indications where CMR is superior to echo and should be regularly used when the information is essential for patient management. Cardiac catheterization is now reserved for resolution of specific anatomical and physiological questions or for intervention.
-
Significant changes to the recommendations for prevention of infective endocarditis (IE); eg, antibiotic prophylaxis is currently only recommended for patients with the highest risk of IE who are undergoing the highest risk procedures (only for dental procedures that require manipulation of the gingival or periapical region of the teeth or perforation of the the oral mucosa).
-
Recommendations for targeted PAH therapy.
-
Acknowledgment and guidance on the increasing role of catheter intervention; eg, device closure in atrial and ventricular septal defects and patent ductus arteriosus; stenting in coarctation of the aorta; percutaneous pulmonary valve replacement in tetralogy of Fallot.
-
Indications for valve-sparing aortic root replacement at a lower level of aortic dimensions (45 mm to 50 mm) instead of Bentall at 50 mm to 55 mm.
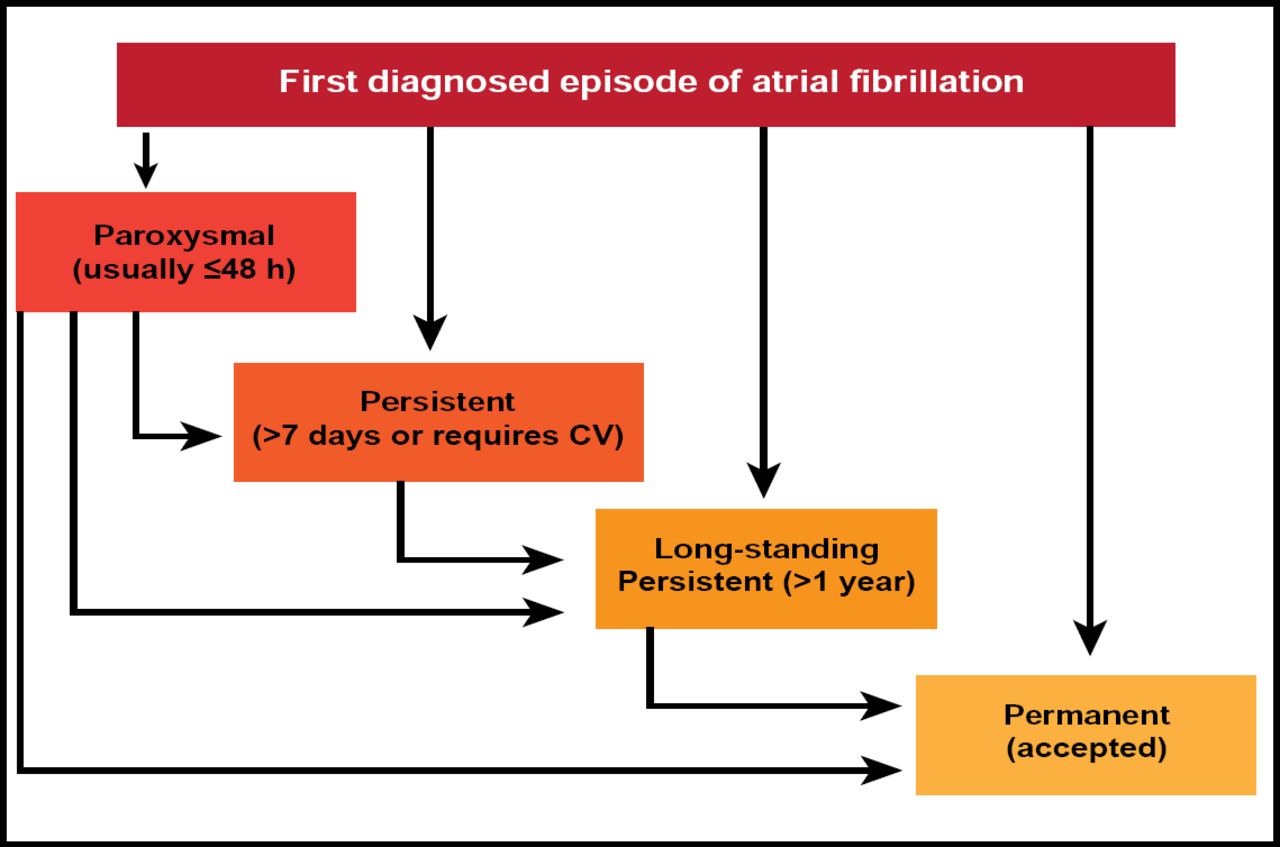
A. John Camm, MD, St. George's University, London, United Kingdom, discussed the first independent ESC Guidelines for the Management of Atrial Fibrillation (AF). Prof. Camm focused on several of the new introductions in the Guidelines, beginning with a repositioning of the classification of AF. Four types are now recognized, including long-standing, persistent AF, defined as AF that has lasted for ≥1 year, and clarification for paroxysmal AF, which is generally self-terminating, usually within 48 hours (Figure 1). It is also recommended that patients with AF be classified based on their EHRA score (Table 3; Class 1: Level B).

Classification of AF.
Reproduced with permission the European Society of Cardiology.
Symptom Score.
The 2010 Guidelines introduce a new scoring system for thromboembolic risk—the CHA2DS2-VASc Score—which includes three new risk factors: vascular disease, age 65 to 74 years, and female gender [Lip GY et al. Chest 2010] and has a point score of 2 for age ≥75 years (vs 1 in the CHADs Score). The maximum score is 9.
Of the numerous recommendations concerning oral anticoagulation therapy (OAC), Prof. Camm focused on two:
-
Antithrombotic therapy to prevent thromboembolism is recommended for all patients with AF, except in those with lone AF, who are aged <65 years, or have contraindications (Class 1: Level A).
-
Combination therapy with aspirin 75–100 mg plus clopidogrel 75 mg daily should be considered for stroke prevention in patients who refuse OAC therapy or when there is a clear contraindication to OAC therapy and a low risk of bleeding (Class 11a: Level B).
The Guidelines now recommend the use of the HAS-BLED Score [Pisters R et al. Chest 2010] to determine bleeding risk.
As in previous guidelines, the primary management for patients with AF is rate control using a lenient strategy for patients who remain asymptomatic and a more strict approach for symptomatic patients (Both Class IIa: Level B).
The following antiarrhythmic drugs are recommended for rhythm control in patients with AF, depending on underlying heart disease: amiodarone, dronedarone, flecainide, propafenone, d, I-sotalol (all Class 1: Level A).
All of the guidelines that are mentioned above are available on the ESC website, http://www.escardio.org/guidelines, and were also published online in the Eur Heart J August 29, 2010.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.