

Summary
Cardiovascular disease (CVD) presents many clinical challenges, which may vary by region or culture due to differences in lifestyle, treatment options, and opportunities for prevention. This article discusses these worldwide disparities in CVD.
- Myocardial Infarction
- Prevention & Screening
Cardiovascular disease (CVD) presents many clinical challenges, which may vary by region or culture due to differences in lifestyle, treatment options, and opportunities for prevention. Annika Rosengren, MD, PhD, University of Gothenburg, Gothenburg, Sweden, discussed these worldwide disparities in CVD.
Most of the causes of coronary heart disease (CHD) are related to lifestyle, and many of these risk factors are modifiable. According to the multinational (52 countries, representing every inhabited continent) INTERHEART study, the 9 major CHD risk factors are raised ApoB/ApoA1 ratio, smoking, hypertension, diabetes, abdominal obesity, psychosocial factors, physical inactivity, inadequate fruit and vegetable consumption, and alcohol consumption. These common modifiable risk factors account for 90% of myocardial infarctions (MIs) [Yusuf S et al. Lancet 2004]. These findings offer some hope, because they demonstrate that CHD and related mortality can be prevented. These data can also be used to develop better treatment strategies and improve survival outcomes.
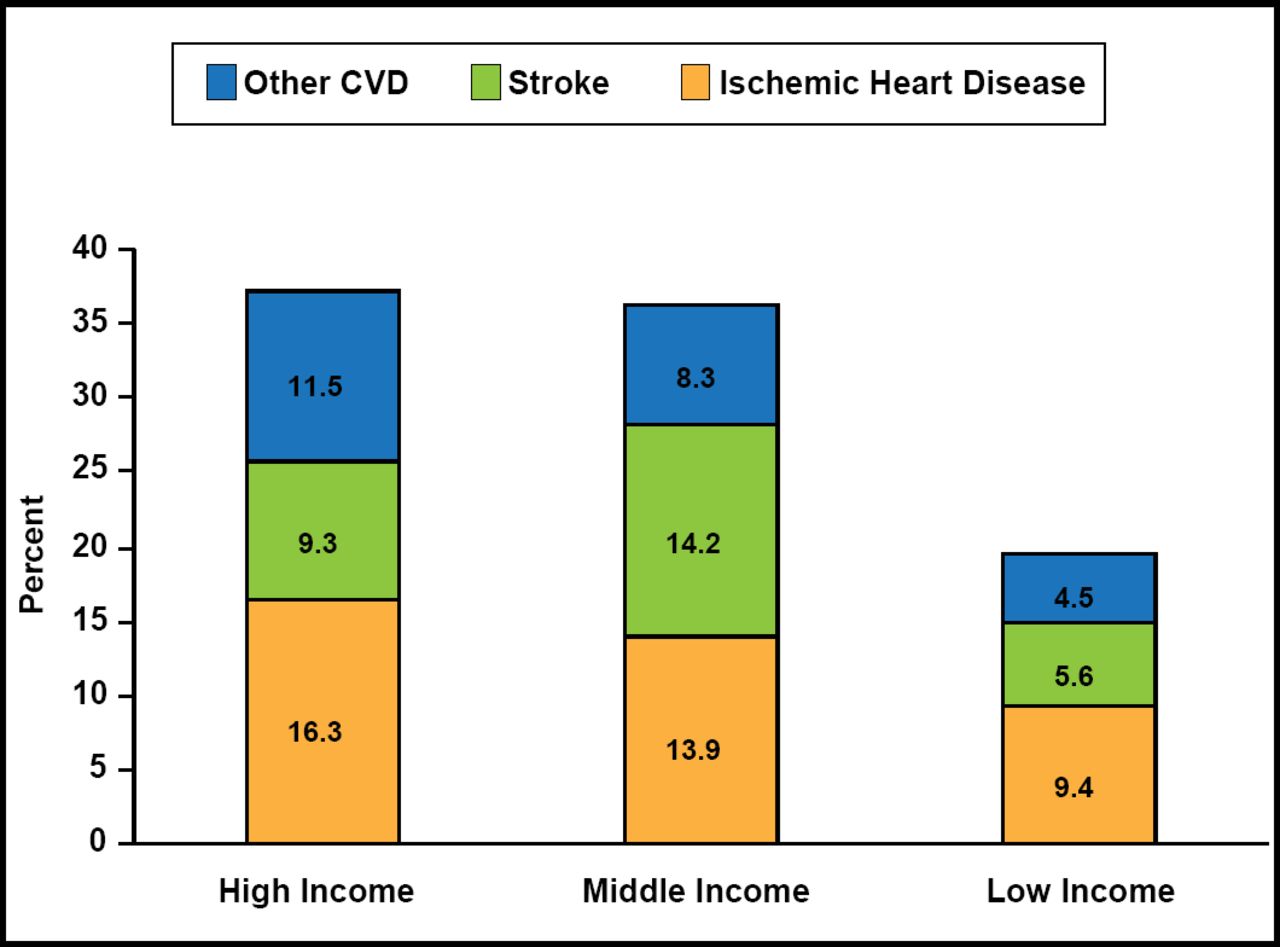
In the United States-based ARIC study, there was a significant decline in severity of MI from 1987 to 2002, as defined by initial ST-segment elevation (p=0.0002), any major Q wave, abnormal biomarkers, and median maximal CK-MB (p<0.0001 for all three) [Myerson M et al. Circulation 2009]. Unfortunately, while the burden of disease appears to be improving in higher-income regions, such as Western Europe, the United States, Canada, and parts of the Western Pacific and the Eastern Mediterranean, continued increases in CHD have been observed in low- and middle-income countries, locations where the majority of the world's population resides (Figure 1). Additionally, where the incidence of CHD declined in younger patients (aged <65 years) in Europe between 1980 and 2006, the incidence has plateaued among the subset who developed CHD below the age of 45 years, which raises concerns about stagnation in CHD treatment and prevention in this population [European Cardiovascular Disease Statistics 2008; O'Flaherty M et al. Heart 2008]. These data suggest that the CHD epidemic is not being properly controlled currently, although this trend could be reversed by timely intervention. Often, by the time CHD symptoms are apparent, the disease is at an advanced stage. Thus, the cost of complacency is high.

Proportion of Deaths Due to CVD by Country Income Level.
Reproduced with permission from the WHO.
Heart failure after acute MI and stroke remain prevalent worldwide. However, the incidence, and morbidity and mortality rates that are associated with CHD and acute MI can be improved, as demonstrated in Sweden and Finland. In the Swedish population between 1987 and 2002, 28-day case fatality in hospitalized patients with acute MI decreased for all age ranges (35 to 54, 55 to 64, 65 to 74, and 75 to 84 years) [Dudas K et al. Eur J Cardiovasc Prevention & Rehabilitation 2006]. The use of medications, such as aspirin, β-blockers, ACE inhibitors, and statins, prior to hospitalization in patients with a first acute MI was associated with a decrease in risk of ST-elevation MI presentation, which also contributed to the decreased incidence of CHD mortality in Sweden [Bjorck L et al. Arch Intern Med 2010]. Further analyses of these mortality trends revealed that out-of-hospital mortality rates from CHD within 28 days were much higher than those reported in-hospital and within reach of therapy [Dudas K et al. Eur J Cardiovasc Prevention & Rehabilitation 2006]. This difference may also explain epidemiological disparities that were identified with CHD in lower- to middle-income countries, as therapy is less readily available in these areas and hospitals are not as accessible.
A cross-sectional Swedish study, investigating risk factors and acute MI in 50-year-old men, found that changes in risk factors correlated with a >50% decline in MI rate over the course of 4 decades (1963 to 2003). While smoking rates, mean serum cholesterol levels, and blood pressure decreased during this time period, an increase in other modifiable risk factors, particularly those related to body size, were observed [Wilhelmsen L et al. J Intern Med 2008]. Weight, waist circumference, and body mass index increased in this cohort between 1963 and 2003 (75.9 vs 84.8 kg, 87 vs 95 cm, and 24.8 vs 26.4 for BMI, respectively; p=0.00001 for trend). Despite progress being made in some high-risk areas, obesity remained a problem, according to this study (obesity rates went from 6.0% in 1963 to 13.8% in 2003).
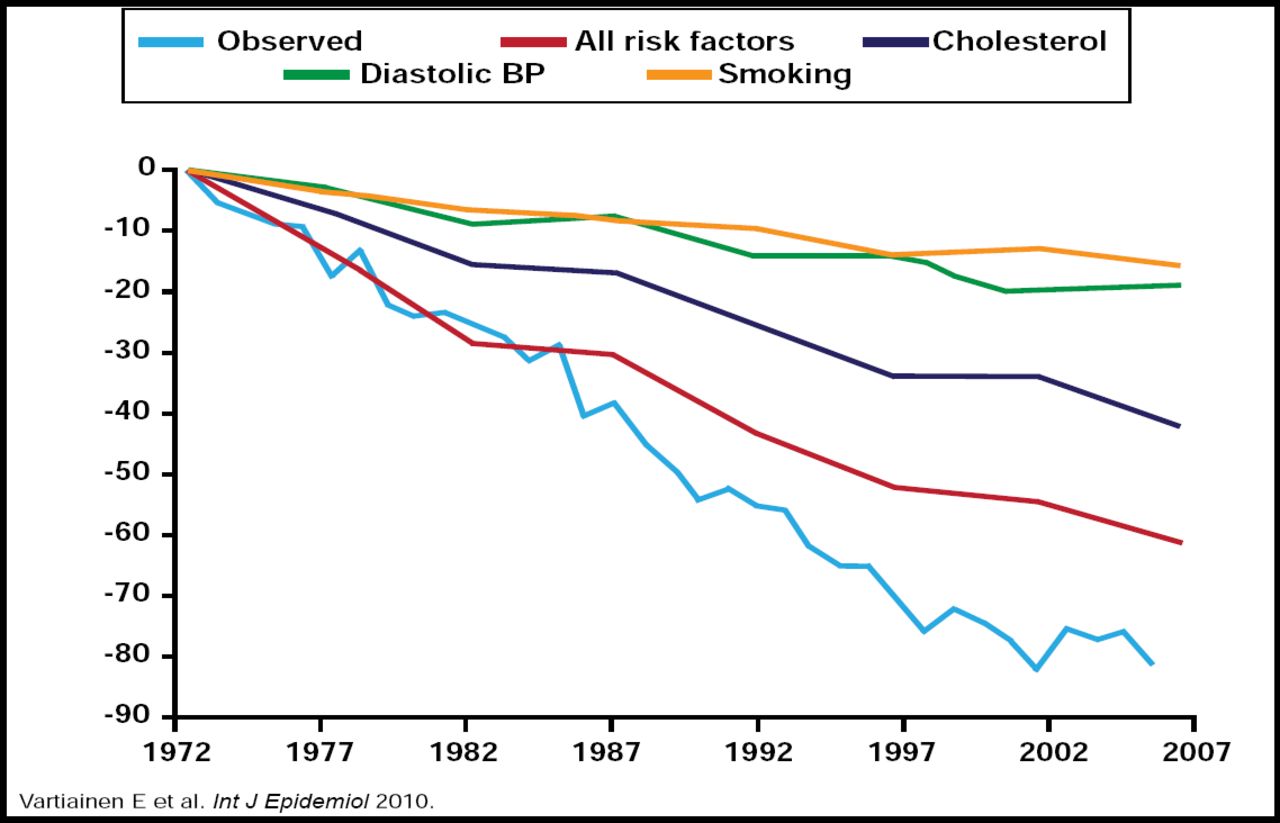
A large study that took place in Finland from 1972 to 2007 also showed promising results over time and demonstrated the profound impact that lifestyle changes and risk factor modification can have on CHD rates. CHD mortality among Finnish males was highest in the world in the late 1960s, resulting in a call to action (The North Karelia Project). In this 35-year study, mean serum total cholesterol declined (21% decrease in men and 23% decrease in women), as did blood pressure levels. (mean decrease in diastolic blood pressure was 8.7 mm Hg). The prevalence of smoking decreased among men throughout the duration of the study but increased among women until 2002, at which point it leveled off. Risk factor changes explained a 60% reduction in CHD mortality among middle-aged Finnish men (Figure 2), with an increase in the reduction after 1987, however, coinciding with the introduction of effective treatment of MI. Similar to the Swedish findings, obesity increased between 1972 and 2007 [Vartiainen E et al. Int J Epidemiol 2010].

Observed and Predicted Decline in CHD Mortality in Men in Finland: 1972–2007.
Reproduced with permission from Oxford University Press.
Prof. Rosengren attributed several preventive strategies and alterations in lifestyle/cultural habits to the improvements that were observed in Finland. Finland had community-based disease prevention and health promotion activities in place, which likely contributed to favorable data in the Finnish study. Increasingly strict tobacco legislation, including the prohibition of all forms of tobacco advertising, sales restrictions for minors aged under age 18 years, and smoking bans in public indoor areas and workplaces, also played a role in risk reduction in Finland. Changes in diet resulted in a decline in saturated fat (22% of energy intake in 1972 to 13% in 2007) and salt intake in that region. The combination of these factors resulted in improved coronary outcomes over time, as reflected by an 80% decline in coronary mortality in middle-aged men [Vartiainen E et al. Int J Epidemiol 2009].
Prof. Rosengren also elaborated on the obesity paradox. How is it that CHD mortality rates continue to fall in the setting of rising rates of obesity? Based on results from the study that was performed in Sweden over a period of 40 years, obese Swedish men who are now in their 50s have lower levels of other CHD risk factors compared with men of 40 years ago in the same age range. Though overall BMI has increased in this cohort (net increase in BMI from 24.8 to 26.4; p<0.0001), this risk is accompanied by higher rates of nonsmoking (OR, 3.39; 95% CI, 1.56 to 7.36), normotension (OR, 2.67; 95% CI, 1.23 to 5.83), and favorable cholesterol levels (OR, 8.30; 95% CI, 2.37 to 29.0) [Rosengren A et al. J Intern Med 2009]. Improved treatment has also contributed to improvements in CHD rates but to a lesser degree than lifestyle modification (decrease in CHD mortality of 36% vs 55%, respectively) [Bjorck L et al. Eur Heart J 2009].
Increases in diabetes and obesity remain a concern and merit further attention. As demonstrated with many of these examples, CHD is preventable, and lifestyle changes, and proactive approaches to CVD management and prevention can lead to improved outcomes. More research into societal determinants of lifestyle and their effects on individual behavior, as well as the impact of lifestyle on risk factors and disease progression, is warranted to develop realistic, cost-effective ways to diminish the global burden of CVD.
- © 2010 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.