

Summary
Obesity (body mass index =30 kg/m2) is increasing globally and is now recognized as a major public health epidemic because of its association with precursors to cardiovascular complications, such as dyslipidemia, insulin resistance, and hypertension.
- Obesity
- Prevention & Screening
Obesity (body mass index [BMI] ≥30 kg/m2) is increasing globally and is now recognized as a major public health epidemic because of its association with precursors to cardiovascular (CV) complications, such as dyslipidemia, insulin resistance, and hypertension.
Twin and adoption studies have shown that ≤70% of the interindividual variance in fat mass is determined by genetic factors, said Professor Amaia Rodrigues Murueta-Goyena, PhD, Clinical Universida de Navarra, Madrid, Spain. Monogenic obesity, a single gene mutation, is extremely rare. Five genes that are linked to monogenic obesity have been associated with early onset obesity, as well as behavioral, developmental, and endocrine disorders. Thirteen genes that are linked to syndromic chromosomal disorders, also rare, have been associated with obesity, mental retardation, dysmorphic features, and organ-specific developmental abnormalities. More commonly, single nucleotide polymorphisms make an individual susceptible to environmental factors that promote energy consumption over energy expenditure. “Genetic strategies can be useful tools to understand the complex molecular and physiologic mechanisms involved in the regulation of body weight,” said Prof. Rodrigues Murueta-Goyena.
Professor Robert Ross, PhD, Queens University, Kingston, Ontario, Canada, discussed the relationship between waist circumference (WC) and BMI, noting that together they characterize a high-risk obesity phenotype for predicting cardiovascular disease (CVD) and diabetes. Although the measurement of BMI is well established, there is no clear measurement protocol for WC. World Health Organization and National Institutes of Health panels recommend protocols that use bony landmarks to guide measurement and that can be easily implemented by both the general public and primary care physicians. Prof. Ross concluded by saying, “We need to rethink our approach to CVD prevention” The primary care physician needs to identify which patients are at high risk for developing CVD, and measuring WC and BMI is an important component in this process.
Professor Luc Van Gaal, MD, Antwerp University Hospital, Belgium, discussed the link between obesity and being overweight and other CVD risks, such as higher triglyceride and glucose levels and a higher incidence of the metabolic syndrome, noting that an association between excess abdominal fat and CV complications has been noted in diabetics.
Insulin resistance, a core symptom of diabetes, is influenced by a number of bioactive mediators, such as leptin, resistin, and the cytokine TNFα, which are released by adipose tissue or body fat. Adipocytokines, derived from adipocytes, have a central role in the regulation of insulin resistance, as well as many aspects of inflammation and immunity. Recent research suggests that TNFα may play a role in the development of insulin resistance, while high plasma levels of the adipocyte-specific secretory protein adiponectin have been associated with a lower risk of myocardial infarction in men.
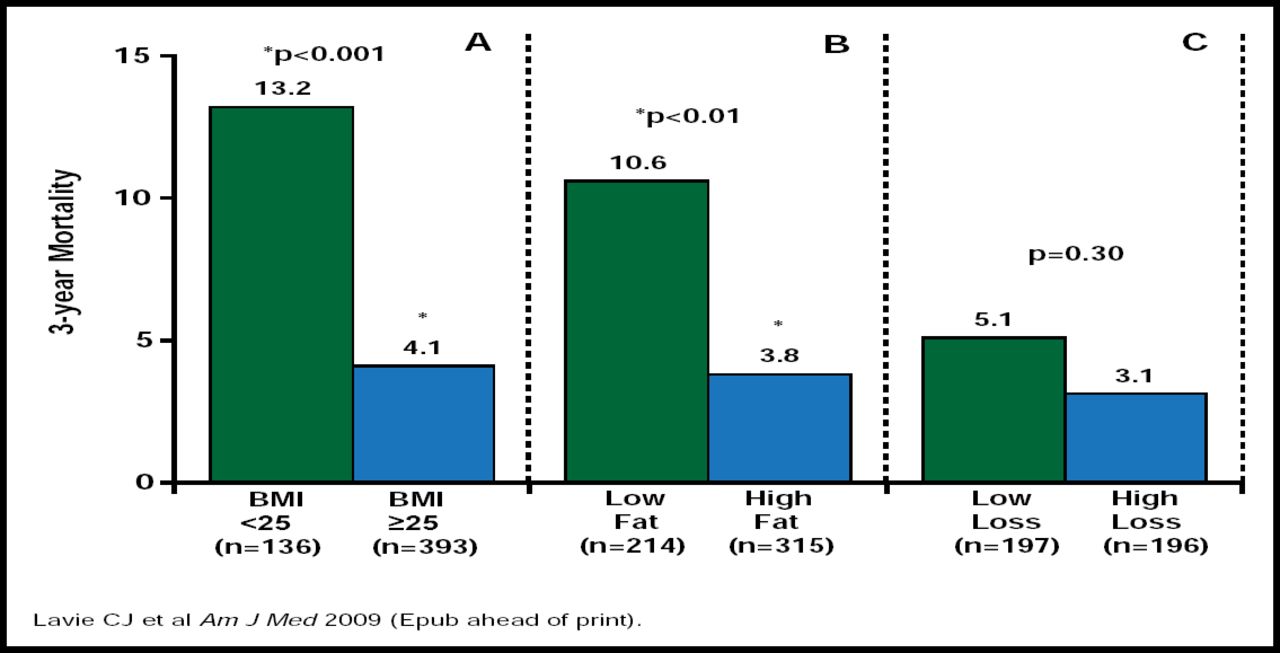
Professor Nicholas Finer, MD, University College London, London, UK, presented data to counter the “obesity paradox” (ie, a higher BMI in people with established CVD is associated with a trend toward improved survival; Figure 1), suggesting that studies that support the paradox may have been flawed, because body wasting, or cardiac cachexia, is a serious complication of congestive heart failure and may have contributed to involuntary weight loss. He said that there is no clear evidence that marked obesity (BMI >35 kg/m2) has a protective effect and that BMI is a poor indicator of total body fat, because body weight is affected by fluid retention. Prof. Finer presented data that showed that weight reduction of as little as 5% improved CV risk, prevented type 2 diabetes, improved quality of life, and improved mechanical symptoms (eg, knee osteoarthritis) and that a >10% reduction in weight improved sleep apnea and lung function in patients with asthma and decreased mortality rate.

Is There a Mortality Paradox?
Reproduced with permission by N. Finer.
Early results from the SCOUT (Sibutramine Cardiovascular OUTcomes) trial active run-in period showed significant benefits (p<0.001) for antiobesity drugs in hypertensive patients. Not only were body weight and WC reduced but systolic blood pressure dropped by a mean of 3.0 mm Hg and diastolic fell by 1.0 mm Hg. Effective weight loss is also achievable with bariatric surgery. After surgery, long-term total mortality is significantly reduced, particularly deaths from diabetes, heart disease, and cancer.
Prof. Finer concluded that active weight management should be a core component of CV management.
- © 2009 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.