

Summary
Pacing both ventricles of the heart, rather than pacing the right ventricle only, prevented loss of left ventricular function among patients with sinus node dysfunction or bradycardia due to atrioventricular block, according to findings from the Pacing to Avoid Cardiac Enlargement [PACE] trial [CUHK_CCT00037].
- Arrhythmias Clinical Trials
Pacing both ventricles of the heart, rather than pacing the right ventricle only, prevented loss of left ventricular function among patients with sinus node dysfunction or bradycardia due to atrioventricular (AV) block, according to new findings from the Pacing to Avoid Cardiac Enlargement (PACE) trial (CUHK_CCT00037).
Right ventricular apical (RVA) pacing is associated with deleterious effects on left ventricular systolic function and adverse clinical outcomes, including progression to heart failure, in patients with standard pacing indications. By comparison, biventricular (BiV) pacing has been shown to slow or reverse progressive adverse ventricular remodeling in certain patients, such as those with heart failure. The PACE trial was designed to evaluate whether BiV pacing is superior to RVA pacing in preserving left ventricular systolic function and avoiding adverse left ventricular structural remodeling in patients with normal left ventricular ejection fraction (LVEF).
Cheuk-Man Yu, MD, Chinese University of Hong Kong, Hong Kong, China, presented results from the PACE trial, which were simultaneously published online in The New England Journal of Medicine.
The PACE trial included 177 patients with a normal LVEF (>45%) who had sinus node dysfunction or AV block. Patients were randomly assigned to BiV (n=89) or RVA (n=88) dual-chamber pacing. The primary endpoints were LVEF and left ventricular end-systolic volume (LVESV) at 12 months.
Baseline characteristics were similar in both treatment groups. In the BiV pacing group, the mean age was 69 years, LVEF was 61.9%, and the indication for pacing was advanced AV block in 55% of patients and sinus node dysfunction in 45% of patients.
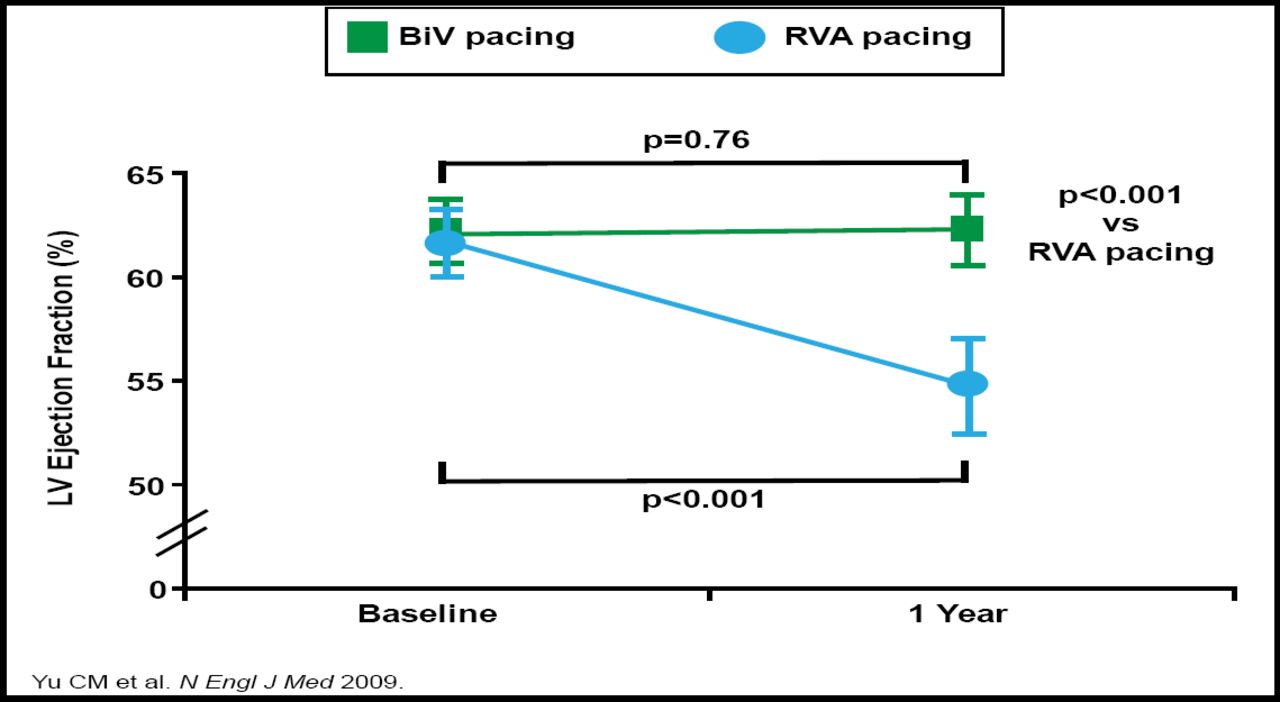
During the first year, LVEF fell in the RVA group but remained unchanged in the BiV group, leading to an absolute difference of 7.4% between groups at 12 months (p<0.001; Figure 1). Fewer patients in the BiV group than in the RVA group experienced a decline in LVEF to <45% (1% vs 9%; p=0.02). At 12 months, LVESV was significantly lower in the BiV group than in the RVA group (27.6 ml vs 35.7 ml; p<0.001), reflecting a relative change from baseline that was 25% greater in the RVA group than in the BiV group (p<0.001).

LVEF at 12 Months.
Copyright © 2009 American Medical Association. All rights reserved.
According to a subgroup analysis, patients benefited from BiV pacing relative to RVA pacing regardless of baseline left ventricular diastolic function. Indeed, the subgroup analysis favored BiV patients in all subgroups, including those who were defined by pacing indication; age; gender; QRS duration; or comorbid hypertension, diabetes, or coronary artery disease.
No significant differences between the two groups were observed in left ventricular end-diastolic volume (p=0.25), 6-minute walk distance (p=0.81), quality of life (p=0.75), or heart failure hospitalizations (p=0.74) at 12 months.
The role of BiV pacing devices, which are more expensive and require more expertise to implant than RVA devices, remains controversial. In an editorial that accompanied the PACE trial, Bruce D. Lindsay, MD, Cleveland Clinic, Cleveland, OH, suggested that BiV pacing may not be appropriate first-line treatment for all patients with high-grade AV block. Instead, patients may be successfully managed with standard RV dual-chamber pacing, monitored with annual echocardiograms, and converted to BiV pacing only when a clinically significant change in LVEF or functional capacity occurs.
- © 2009 MD Conference Express
Additional Reading
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.