

Summary
This article discusses the future of cardiac imaging: changes that favor the use of echocardiography (ECHO), important indications for non-invasive imaging (the ability to provide a work-up of new onset heart failure and chest pain, risk stratification in suspected CAD, and assessment of myocardial viability), the benefits of sequential imaging for diagnosing ischemic heart disease, and current challenges in imaging.
- cardiac imaging techniques
- imaging modalities

Thomas H. Marwick, PhD, Princess Alexandra Hospital, Brisbane, Australia, discussed changes that favor the use of echocardiography (ECHO).
Easier to use, handheld ECHO devices that are appropriate for office and bedside diagnoses, already have proven to be useful in providing additional diagnostic and prognostic information in the examination of patients who have a low likelihood of myocardial ischemia or infarction and symptoms that are suggestive of acute coronary syndrome [Weston P et al. Am Heart Journal 2004]. However, better training guidelines, competency evaluation, and adoption of a uniform method for computer quantification of myocardial imaging are needed if these devices are to be used by non-echocardiographers for clinical decision-making [De Cara J et al. Eur J Echo 2003].
As a diagnostic tool, ECHO faces some challenges, which may be overcome through technological development. Two-dimensional strain (novel software for real-time quantitative ECHO assessment of myocardial function) may reduce subjectivity, address the need to identify cardiac problems earlier, and resolve some training issues [Leitman M et al. J Am Soc Echocardiogr 2004]. High frame rate 3D imaging should improve the accuracy and reproducibility of quantitative ECHO measurements and the success rate of early diagnoses.
There also is good evidence that real-time contrast improves sensitivity of dobutamine stress echocardiography and may provide incremental prognostic information for patients with known or suspected coronary artery disease (CAD) [Tsutsui JM et al. Circulation 2005]. Experiments are ongoing using microbubbles in contrast agents. Microbubbles that are cavitated with ultrasonography can be used to dissolve blood clots or deliver drugs [Unger EC et al. Eur J Radiol 2002].
The meshing of automation, minimization, and 3D imaging will ensure the expanding use of ECHO, Dr. Marwick concluded.
Heiko Mahrholdt, MD, Robert-Bosch Krankenhaus, Stuttgart, Germany, noted that important indications for non-invasive imaging include the ability to provide a work-up of new onset heart failure and chest pain, risk stratification in suspected CAD, and assessment of myocardial viability. Cardiac magnetic resonance (CMR) provides the ultimate one-stop diagnostic evaluation and can provide information that concerns morphology, function, valvular assessment, myocardial perfusion, and non-invasive tissue characterization based on detection of myocardial edema, necrosis, and scarring. In severe ischemic heart failure, CMR identifies areas of decreased flow, metabolism, and myocardial edema, as well as PET, but identifies scar tissue more frequently [Cury RC et al. Circulation 2008].
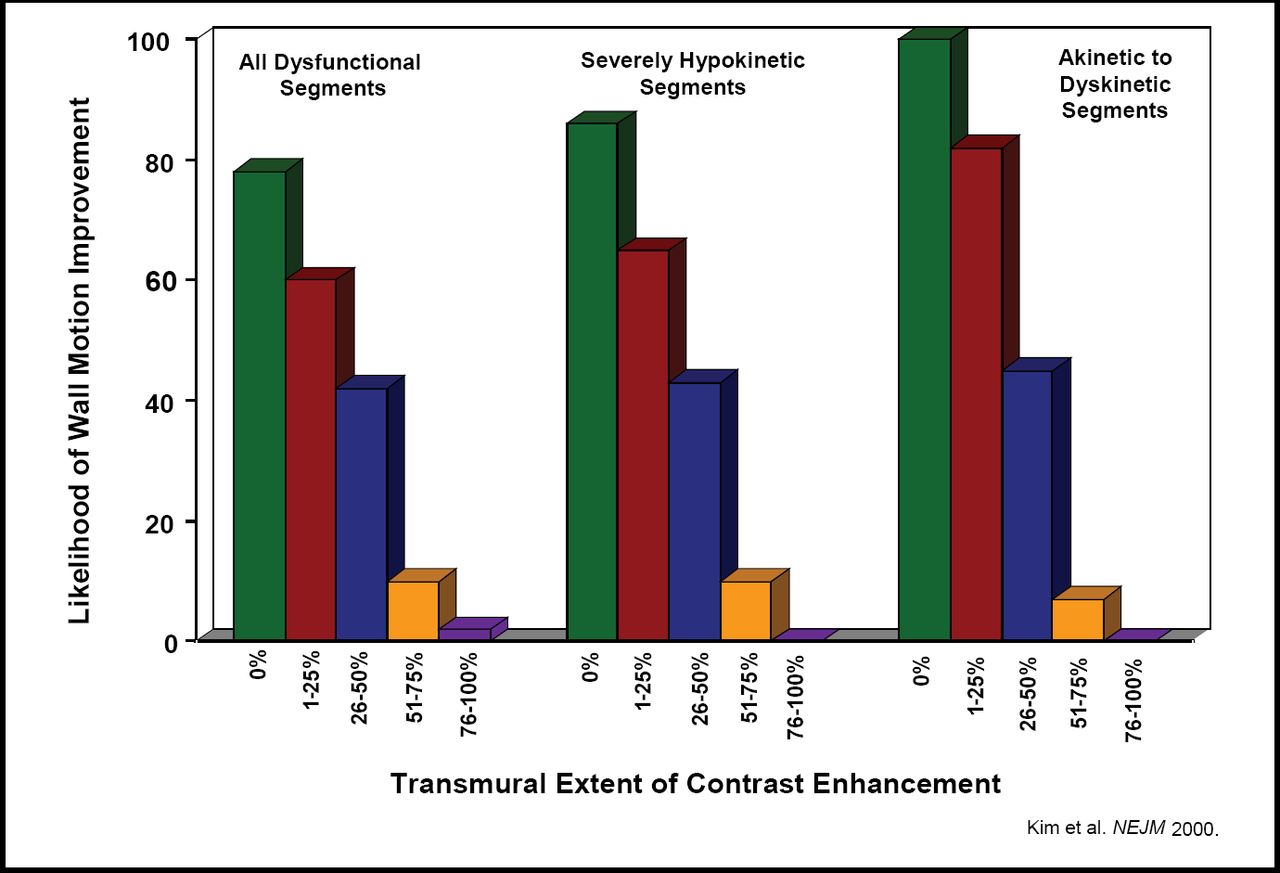
CMR has higher spatial resolution than single photon emission computed tomography (SPECT) and can detect subendocardial infarcts that SPECT misses [Wagner A et al. Lancet 2003]. CMR can be used to distinguish between reversible and irreversible myocardial ischemic injury, predict improvement after revascularization [Kim RJ et al. N Engl J Med 2000], and has the best reproducibility of all non-invasive imaging techniques [Mahrholdt H et al. Circulation 2002] (Figure 1).

Relation Between the Transmural Extent of Hyperenhancement Before Revascularization and the Likelihood of Increased Contractility After Revascularization.
CMR could replace SPECT in many trials that use “infarct size” as an endpoint. The combination of cine, contrast, and perfusion CMR has the potential to overcome many limitations (sensitivity, specificity and accuracy) of other techniques that currently are used in clinical settings and emergency rooms, although the limited availability and costs of CMR remain challenges (Table 1).
Comparison to Other Techniques.
However, Prof. Mahrholdt concluded, although CMR may address questions that are not answered by ECHO, ECHO will remain the first-line imaging method that is used at the bedside in 2020, and the use of SPECT, coronary CT, and diagnostic coronary angiograms will decrease. Frank M. Bengel, MD, Johns Hopkins Medical Institutions, Baltimore, MD, outlined the challenges for cardiac imaging starting from the belief that current imaging markers are not sufficient to meet the diagnostic needs of cardiovascular medicine in the future. He sees the need for imaging technologies that can detect the earliest stages of CAD in order to reverse or prevent disease progression, characterize disease on a more individual basis, monitor therapeutic intervention, and predict outcome. Although a number of technologies can image the myocardial disease process at the tissue, pathophysiologcal and morphological level, experimental studies have shown the feasibility of doing this at the molecular level, utilizing different cardiac molecular imaging targets.
The integrins, a family of transmembrane receptor proteins that are composed of alpha and beta chains of heterodimeric adhesion molecules and found on almost all cell types, are involved in thrombus formation, matrix activation, inflammation and angiogenesis.
An in vivo PET imaging approach that uses an 18F-labeled alphavbeta3 integrin antagonist (18F-Galacto-RGD) to monitor integrin expression after myocardial infarction appears to hold promise for monitoring the post-ischemic myocardial repair processes [Higuchi T et al. Cardiovasc Res 2008]. The AT1 radioligand receptor (AT1R), which mediates mitogenic, proinflammatory, proapoptotic, and profibrotic processes in stress conditions, also may be a target for molecular imaging in the heart [Zober TG et al. Nucl Biol 2006].
Several approaches that are aimed at identifying plaque inflammation, apoptosis, smooth muscle cell proliferation, extracellular matrix activation, oxidative stress, or platelet binding are being studied. For example, simvastatin has been shown to attenuate plaque inflammation as detected by 18F-fluorodeoxyglucose positron emission tomography (18FDG-PET), coregistered with computerized tomography [Tahara N et al. J Am Col Cardiol 2006].
Molecular imaging approaches are fast emerging for identification of biologic targets that are associated with early disease that will be useful as a guide to treatment that is based on individual biology. To make molecular imaging a reality in 2020 there is a need for a successful translation of these experimental techniques to the clinic, multi-disciplinary collaboration, and the integration of molecular medicine and therapy efforts. “Increasing specificity of therapeutic and preventive measures requires increasing specificity of diagnostic tools,” concluded Dr. Bengel.
Frank E. Rademakers, MD, Catholic University, Leuven, Belgium, discussed the benefits of using sequential imaging techniques for diagnoses of ischemic heart disease. “We need to focus on what we need to do, rather than on what we can do,” he said. “We already know that if we can identify myocardial ischemia in a large territory and treat it using percutaneous coronary intervention or surgery early enough, the long-term risk of a major cardiac event can be reduced.”
Since the 1980′s, there has been an increase in the use of invasive cardiology and ECHO, little change in the use of stress and nuclear testing, and a decrease in the use of Swan-Ganz catheterization [Pearte CA et al. Am J Cardiol 2008]. There are many potential imaging combinations, eg, CT or MRI with SPECT, PET, and ECHO. He advises demonstrating the benefits of first combining the measurements of these devices before combining the machines, as new techniques are not always helpful to the patient. A number of studies that use new imaging tools show suboptimal results, or predictability, and overlap as to predictive value.
The use of diagnostic and prognostic tools should be balanced by each patient's circumstances, age, and expectations, while taking into consideration the risks, benefits, costs, and effectiveness of the procedure. Functional noninvasive imaging that uses a combination of approaches will play an even greater role as an imaging tool, and techniques that use ionizing radiations will be even more limited in the future. The use of stress cardiac MRI will emerge as an important noninvasive method in the detection of CAD, he concluded.
- © 2008 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.