

Summary
Cardiovascular imaging was chosen as the theme for the European Society of Cardiology Congress 2008. Within this article, international leaders in cardiovascular imaging debated the merits of different imaging tools. The presenters focused on both technical innovations and the implementation of emerging imaging techniques in clinical practice.
- valvular disease
- imaging modalities
- cardiac imaging techniques
Cardiovascular imaging was chosen as the theme for the 2008 European Society of Cardiology (ESC) Congress. In this special highlights session, international leaders in cardiovascular imaging debated the merits of different imaging tools. The presenters focused on both technical innovations and the implementation of emerging imaging techniques in clinical practice.
Resting Echocardiography
James D. Thomas, MD, Cleveland Clinic, Cleveland, OH, noted that resting echocardiography (ECHO) continues to be the cornerstone imaging technique for evaluating valvular diseases. Conventional tools such as two-dimensional transthoracic (TTE) and transoesophageal (TEE) ECHO are useful for characterizing the anatomy of patients with suspected valvular heart disease. More recent techniques, including three-dimensional TTE and TEE, provide better visualization of aortic/mitral stenosis. In addition, three-dimensional TTE and TEE provide more accurate quantification of left ventricular (LV) volume and ejection fraction (EF).
Two approaches for quantifying stenosis have been validated for use in clinical practice. First, assessment of valves using Doppler ultrasonography and the modified Bernoulli equation (gradient = 4 × velocity2) can provide important information about the pressure drop across the stenosis. As blood flows across a stenotic valve, flow must accelerate for the volume to remain constant. Doppler ultrasonography detects this increase in velocity and can be used to estimate the mean pressure gradient across the valve and the degree of stenosis. Second, the continuity equation enables physicians to assess the valve area, most commonly the aortic valve, because the continuity equation states that flow across the left ventricular outflow tract must be the same as the flow across the aortic valve. A valve area of <1.0 cm2 is classified as severe aortic stenosis.
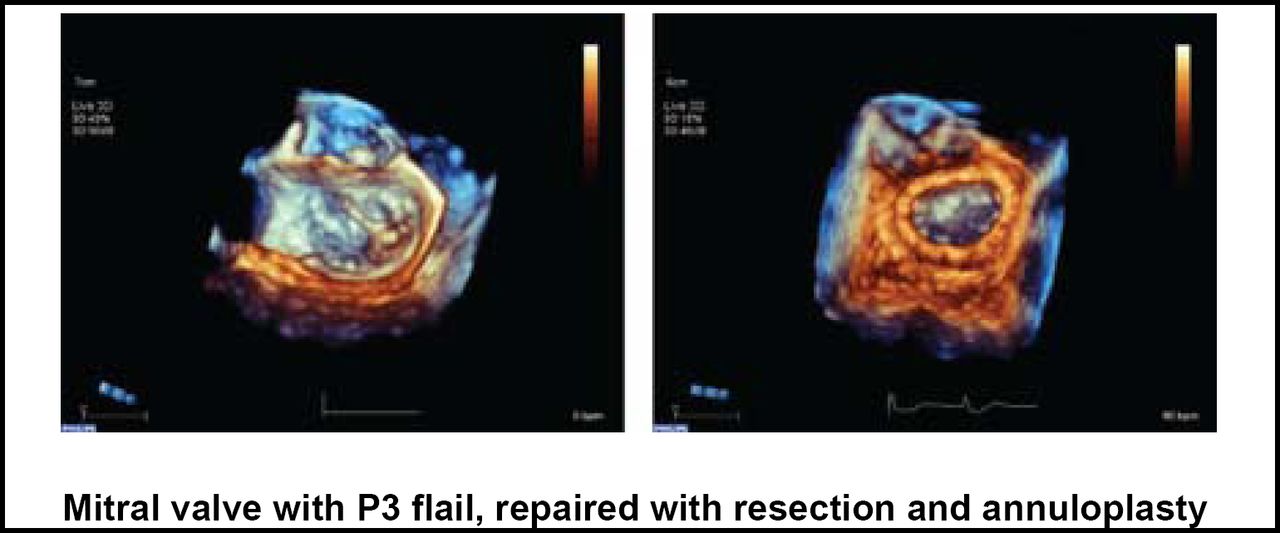
Cardiologists are increasingly using two- and three-dimensional TEE to guide interventions, Dr. Thomas said. For example, these tools are commonly used in the operating room to guide valve repair or myectomy (Figure 1). TEE also is being used in cardiac catheterization laboratories during percutaneous mitral stenosis dilatation, insertion of closure devices, or percutaneous implantation of aortic bioprosthesis in patients with aortic stenosis. For all of these procedures, resting echocardiography is an indispensible tool, Dr. Thomas concluded.

3DTEE in Intraperative ECHO.
Stress Echocardiography
“Given that valve disease is viewed as fairly static, most management decisions are based on resting evaluation,” said Luc A. Pierard, MD, PhD, University Hospital Sart Tilman, Liège, Belgium. However, combined with Doppler ECHO, exercise testing can help to unmask symptoms, determine the level of allowed physical activity, and stratify risk.
Although exercise testing in patients with significant aortic stenosis (AS) may be risky, stress ECHO may be useful in asymptomatic patients, particularly when the severity of AS is in doubt. In the current American College of Cardiology/American Heart Association (ACC/AHA) guidelines on the management of valvular heart disease, stress ECHO may be considered (class IIb recommendation) in selected patients with severe asymptomatic AS [Fuster V et al. Circulation 2006], while exercise testing is currently contraindicated in symptomatic patients with severe AS.
For asymptomatic patients, dobutamine stress ECHO is another option that can provide important diagnostic and prognostic information. For example, an increased pressure gradient with unchanged aortic valve area (AVA) indicates fixed AS, while an unchanged gradient with increased AVA (>0.3 cm2) suggests relative AS [de Filippi CR et al. Am J Cardiol 1995]. In addition, the presence of a contractile reserve is an independent predictor of good outcome following surgery, while prognosis worsens in its absence [Monin JL et al. Circulation 2003].
Stress ECHO also plays a role in the assessment of patients with mitral regurgitation. According to the 2006 ACC/AHA guidelines, exercise Doppler ECHO is reasonable in asymptomatic patients with severe mitral regurgitation to assess exercise tolerance and the effects of exercise on pulmonary artery pressure and mitral regurgitation severity [Fuster V et al. Circulation 2006]. Prof. Pierard noted that this recommendation was not included in the 2007 ESC guidelines.
“Exercise echocardiography allows a comprehensive evaluation of the dynamic component and the hemodynamic repercussions of valve disease,” Dr. Pierard argued. Although functional assessment is not yet mandatory, it provides useful information in appropriate patients, he concluded.
MRI and CT
Jean-Louis J. Vanoverschelde, MD, PhD, University of Louvain, Brussels, Belgium, focused on the use of cardiovascular magnetic resonance (CMR) and computed tomography (CT) techniques to improve the assessment and quantification of valvular abnormalities.
One of the most exciting advances in cardiac imaging is the use of multidetector CT scanning, a form of CT (MDCT) scanning in which the linear array of detector elements that are used in typical conventional scanning is replaced by a two-dimensional array of detector elements, allowing MDCT scanners to acquire multiple images simultaneously, increasing both the speed and resolution of conventional CT scans. In the cardiology setting, MDCT scanning can be used to measure the aortic valve area and detect AS at the time of noninvasive coronary imaging with an accuracy that is similar to that of MRI and TEE [Pouleur AC et al. Radiology 2007].
CT scanning also is being used in the assessment of mitral regurgitation, the most common valve lesion in modern clinical practice. MDCT allows physicians to visualize the morphology of the mitral valve and grade the severity of mitral regurgitation [Alkadhi H et al. Radiology 2006]. By depicting morphologicvalve abnormalities, MDCT provides information about the possible underlying cause and mechanism of regurgitation.
In patients with mitral regurgitation, CMR imaging of the regurgitant lesion provides quantitative measurements that are in good agreement with the accepted invasive and noninvasive methods, such as invasive catheterization and ECHO [Buchner H et al. Circ Cardiovasc Imaging 2008]. CMR is another promising new method for measuring of the precise regurgitant orifice area and severity of mitral regurgitation.
“Both cardiac CT and CMR allow for an accurate assessment of all clinically important aspects of valvular disease,” Prof. Vanoverschelde said. In particular, these techniques are useful in measuring the severity of valve dysfunction and its consequences on LV function. Importantly, CT and CMR also allow for visualization of the coronary anatomy—a benefit that ECHO does not provide.
Given these benefits, cardiac CT and CMR are particularly helpful in difficult cases. These techniques provide valuable information when ECHO has yielded ambiguous findings or in cases when the results of ECHO and physical examination contradict each other.
Summary
Recent advances in cardiovascular imaging have provided physicians with more diagnostic and prognostic information for the assessment of patients with valvular disease. Because imaging is more commonly used to guide interventions, imaging tools are becoming fixtures of the operating room and the coronary catheterization laboratory. When used appropriately, imaging techniques such as resting ECHO, stress ECHO, CMR, and CT can help guide clinical decision-making and improve patient outcomes.
- © 2008 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.