

Summary
This article provides new insights in managing musculoskeletal pain. Patients suffering from fibromyalgia perceive pain differently than healthy subjects, which may be the result of how pain is processed in the brain [Kulkarni et al. Rheum 2005]. State-of-the-art brain imaging techniques are being used to understand the processing of pain associated with fibromyalgia and chronic pain in general [Jones et al. Brit Med Bull 2003].
- fibromyalgia
Professor Anthony Jones, MD, University of Manchester, England, chaired an important session to provide new insights in managing musculoskeletal pain. Patients suffering from fibromyalgia perceive pain differently than healthy subjects, which may be the result of how pain is processed in the brain [Kulkarni et al. Rheum 2005]. State-of-the-art brain imaging techniques are being used to understand the processing of pain associated with fibromyalgia and chronic pain in general [Jones et al. Brit Med Bull 2003].
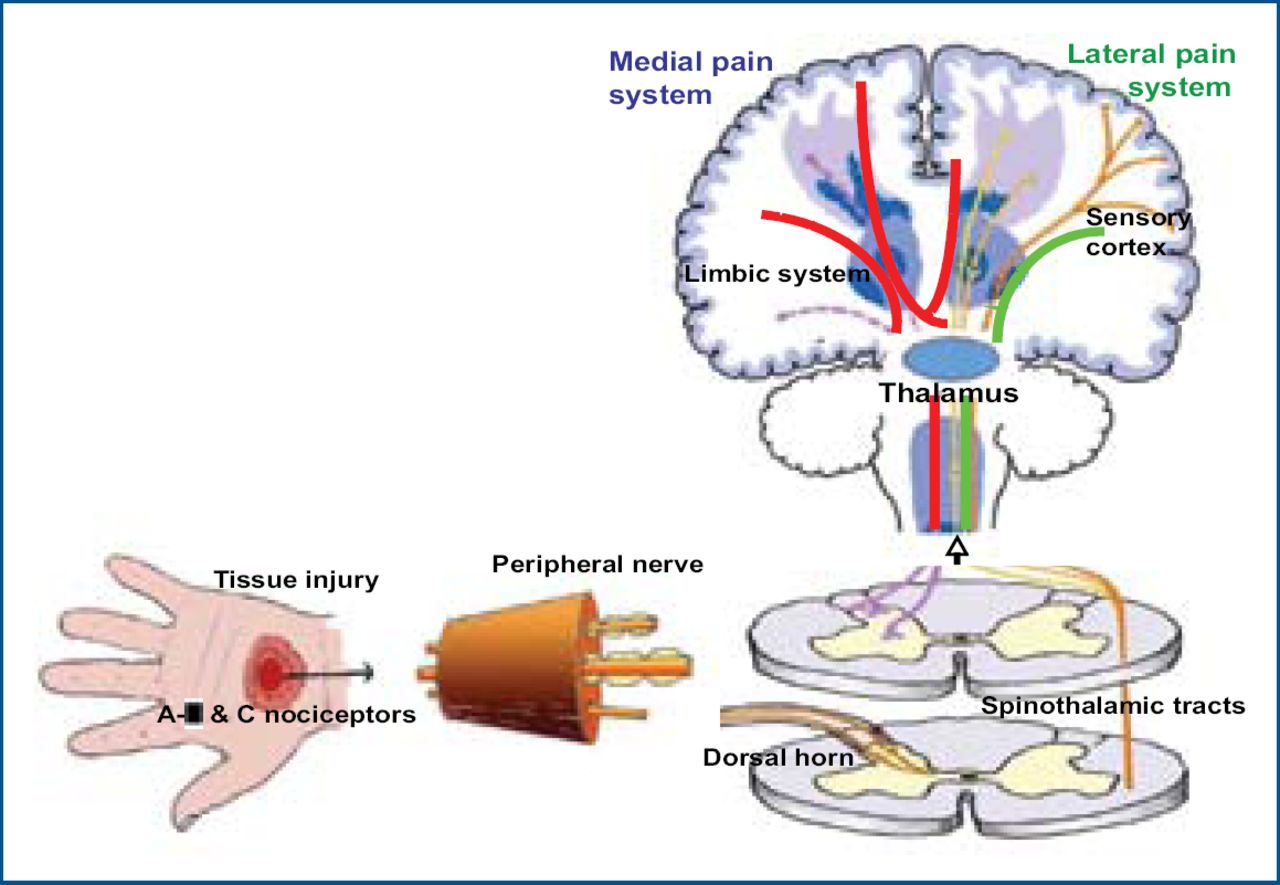
The part of the nervous system associated with pain as a consequence of organ or tissue damage is called the nociceptive system. The currently accepted theory is that there are two networks involved in pain processing in the brain: the lateral nociceptive system, which projects through lateral thalamic nuclei to brain regions including the primary and secondary somatosensory cortices; and the medial nociceptive system, which projects through medial thalamic nuclei to brain regions, including the prefrontal, insula and anterior cingulate cortices (Figure 1).

Pain Pathways.
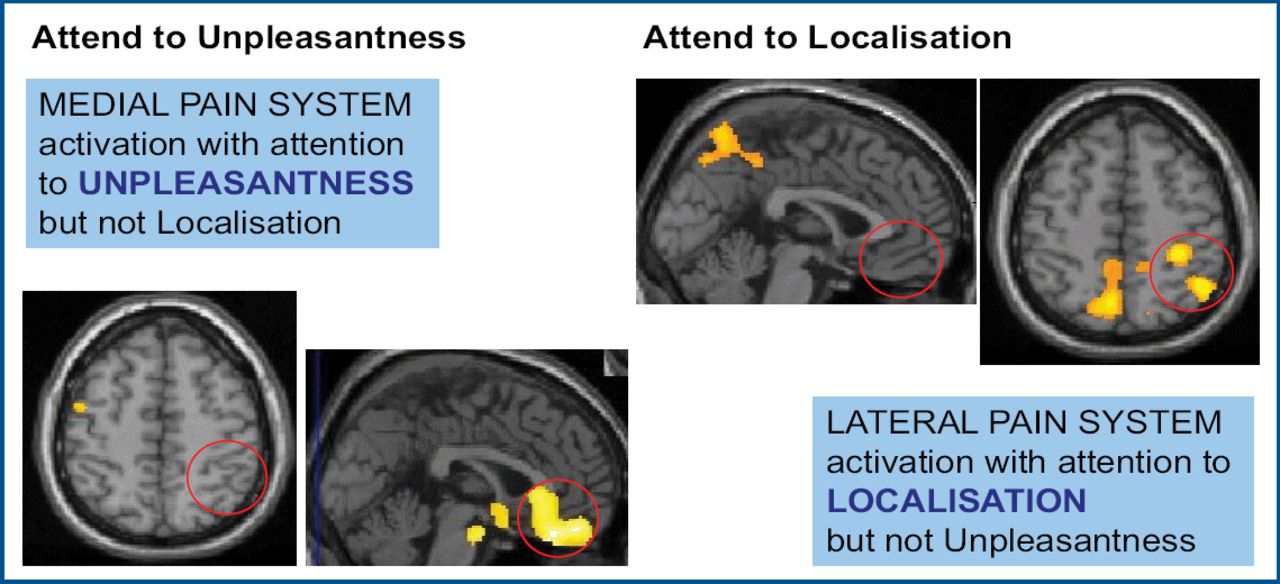
The lateral pain system is thought to be responsible for the sensory aspects of pain such as its location. The medial pain system is thought to be responsible for the emotional aspects of pain, such as how unpleasant it feels. Both can be visualized with PET when activated [Kulkarni et al. Eur J Neurosci 2005]. Understanding the role of these brain areas in anticipation, attention, and emotional responses to pain is the next challenge (Figure 2).

Functions of the Medial and Lateral Pain Pathways.
Chronic pain, however, may also be a result of damage to the nervous system itself, eg, pain after nerve injury, spinal cord injury pain, or post-stroke pain. This type of pain is called neuropathic pain, and occurs as a direct consequence of a lesion or disease affecting the somatosensory system. Nociceptive and neuropathic pain are both sensitive to treatment with opioids, but NSAIDs are more appropriate for nociceptive pain, whereas other substances (eg, anticonvulsants) are appropriate for neuropathic pain. Tricyclic antidepressants can be used as adjunct analgesics for most types of pain. Understanding the differential diagnosis of neuropathic vs nociceptive pain components guides therapeutic decisions in the treatment of chronic pain.
Opioids have an established role in the management of acute pain, pain associated with terminal illness, and as emerging clinical trial data suggests, in the management of persistent non-cancer pain. However, questions remain regarding the efficacy and safety of their use long-term. The risks of opioid treatment include failure to achieve analgesia, constipation, somnolence, dependence, tolerance, respiratory depression, and addiction.
The use of opioids for non-cancer pain (whether short-or long-term) has variable support from the clinical community. Some report failure of the key treatment goals: pain relief, improved quality of life, and improved functional capacity. Opioid use may be associated with reports of moderate/severe pain, poor self-rated health, unemployment, increased use of the healthcare system, and negative influences on quality of life [Eriksen J et al. Pain 2006]. However, other substantial trials have shown clear benefits [Rowbotham et al. New Engl J Med 2003].
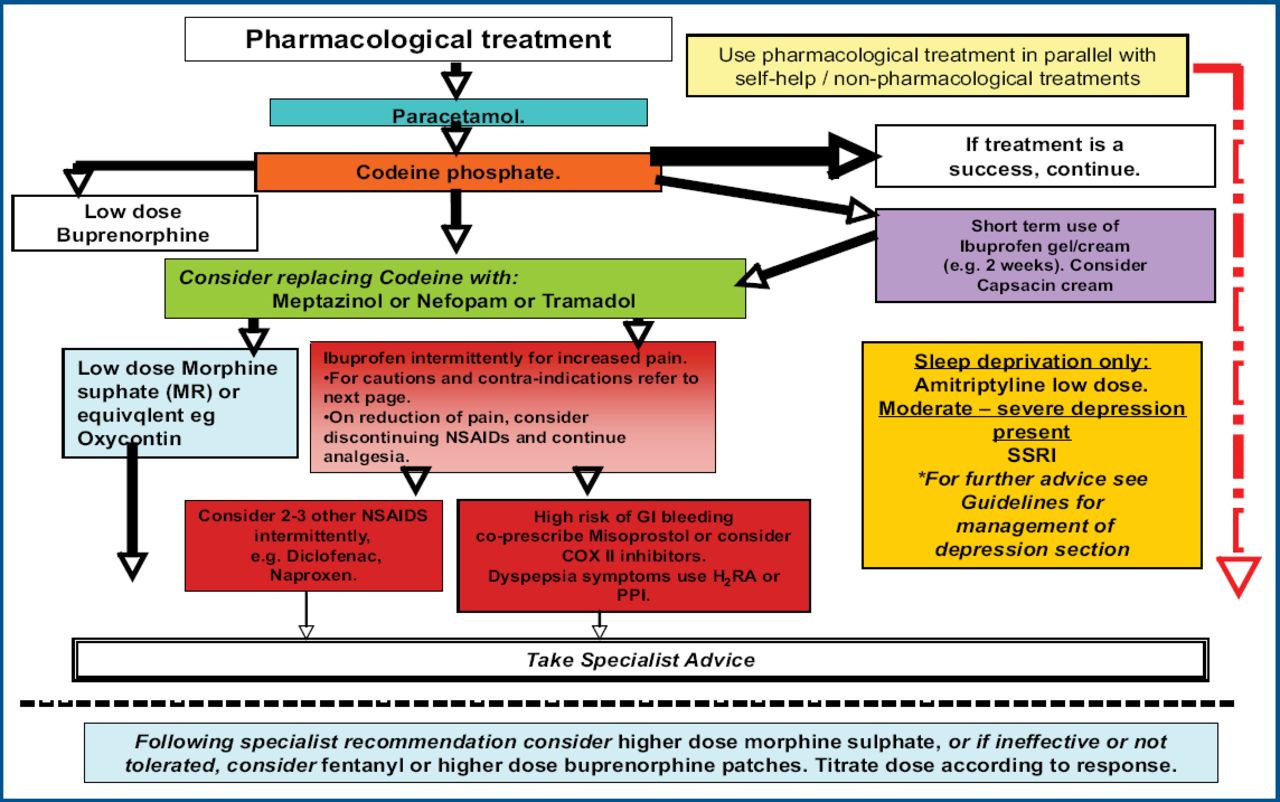
When prescribing opioids for non-cancer pain, known risk factors such as abuse/misuse (eg, genetic, environmental factors, comorbid psychiatric diagnosis, previous history of substance misuse – including alcohol) should be identified and regular re-evaluations of drug efficacy, side effects, and pattern of opioid use should be performed. Treatment recommendations can be found at www.ampainsoc.org/advocacy/opioids.htm (Figure 3).

Treatment Options.
As mentioned in the discussion, the use of mild and stronger opiates in benign pain is very common. Many of these patients suffer from chronic recurrent acute pain, which does not neatly fit into chronic/acute pain categories. There is emerging evidence of cardiovascular risk of prescribing NSAIDS together with the established risks of gut damage, especially in the elderly. There is, therefore, a clear need for more substantial clinical trial data on the use of opiates in well psychologically defined clinical populations to properly assess the relative risks and benefits in these patients.
- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.