

Summary
This article presents the results of a systematic review of 15 studies in early (duration up to 2 years) rheumatoid arthritis (RA) patients (n=1,414 patients), which indicates that glucocorticoids, in addition to standard therapy, can substantially reduce the rate of erosion progression in RA [Kirwan J et al. 2007;1:CD006356].
Professor Maarten Boers, MD, VU University Medical Center, Amsterdam, presented the results of a systematic review of 15 studies in early (duration up to 2 years) rheumatoid arthritis (RA) patients (n=1,414 patients), which indicates that glucocorticoids, in addition to standard therapy, can substantially reduce the rate of erosion progression in RA [Kirwan J et al. 2007; 1:CD006356].
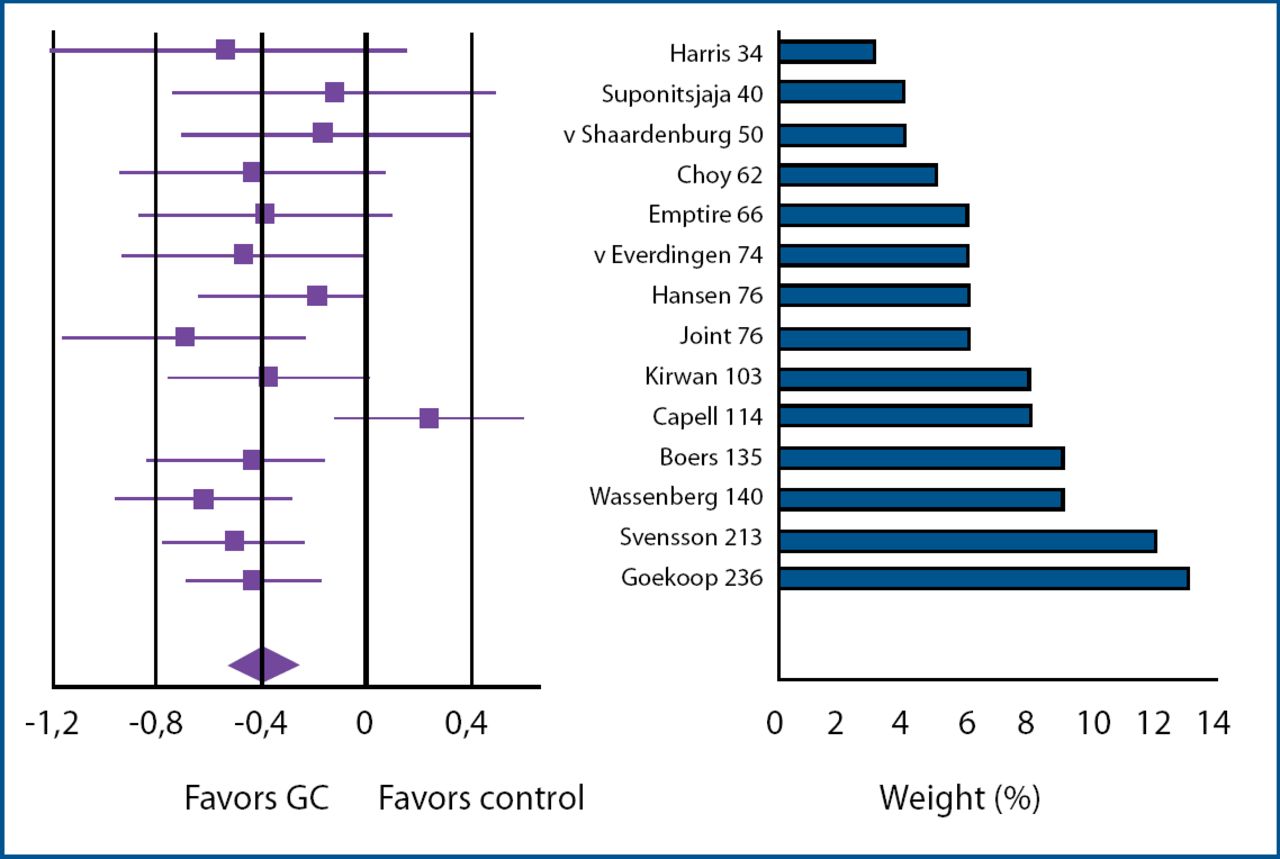
The standardized mean difference in progression was 0.40 in favor of glucocorticoids (95% CI 0.27, 0.54). Of the studies lasting 2 years (n=806 patients), the standardized mean difference in progression in favor of glucocorticoids at 1 year was 0.45 (0.24, 0.66); at 2 years it was 0.42 (0.30, 0.55; Figure 1). All studies except one showed a numerical treatment effect in favor of glucocorticoids.

Standardized Mean Difference in Progression.
Prof. Boers concluded “Even in the most conservative estimate, the evidence that glucocorticoids given in addition to standard therapy can substantially reduce the rate of erosion progression in rheumatoid arthritis is now overwhelming.” Additionally, the long-term structural effects of the oral prednisolone pulse as given in the COBRA schedule suggest true disease modification: permanently improved prognosis regardless of subsequent therapy [Landewé et al. Arthritis Rheum 2002; 46:347–56].
José Antonio P. Da Silva, MD, Hospitais da Universidade de Coimbra, Portugal, presented results of a literature review of the adverse events of long term low-dose glucocorticoid treatment and an analysis of toxicity data from randomized controlled trials of low-dose glucocorticoids in RA patients.
The results indicated that many of the feared adverse events of low-dose therapy are not supported by data and are overestimated by common wisdom [Da Silva JAP et al. Ann Rheum Dis 2006]. “By conventional definition, there is overwhelming evidence that glucocorticoids slow radiological progression by at least 50%,” he concluded. “In the hands of the right people, given on the right schedule with the right monitoring scheme, glucocorticoids are no more, and maybe less, toxic than other DMARDs.”
Treating early RA with one DMARD improves symptoms but has incomplete effects on erosive damage and disability. Ernest H. Choy, MD, King's College London, presented results of the CARDERA study, a 2-year randomized double-blind 2×2 factorial trial in early RA patients. Patients (n=467) were randomly assigned to 4 groups: methotrexate alone, methotrexate+cyclosporin, methotrexate+prednisone, and methotrexate+prednisone +cyclosporine. The target dose of methotrexate was 15 mg/week. Prednisone daily doses were tapered from 60 mg (weeks 1, 2) to 7.5 mg (weeks 7–28) to withdrawal (week 35). Cyclosporine was started 3 months after the start of methotrexate.
The number of patients with new erosions was reduced by ∼50% by adding cyclosporine (p=0.01) or prednisolone (p=0.03); both treatments reduced in Larsen's X-ray scores by >2 units. Triple therapy also reduced disability and improved quality of life.
Dr. Choy concluded, “This study confirms the existence of a “window of opportunity” in early rheumatoid arthritis, when intensive combination therapy produces sustained benefits on damage and disability. Prednisolone and cyclosporin in combination with methotrexate reduce erosive damage independently; they act synergistically to improve physical function and quality of life.”
Frank Buttgereit, MD, Charité University Hospital, Berlin, presented the results of a 3 month randomized, controlled phase 3 study which compared a newly developed modified-release (MR) prednisone tablet (designed to be taken at bedtime) which releases prednisone 4 hours after ingestion with immediate-release (IR) prednisone. The primary outcome measure was patient reported duration of morning stiffness.
A total of 288 RA (mean age 55.0 yrs, 14.2% male, mean disease duration 115.3 months) were randomly assigned to two groups. Treatment with MR prednisone resulted in a significant reduction in the duration of morning stiffness vs IR prednisone (22.7% vs 0.4%; p=0.0226). The study investigators concluded that MR prednisone provides a clinically relevant reduction of morning stiffness added to the known therapeutic effects of IR prednisone.
In summary, the magnitude and longevity of the effect of glucocorticoids on disease activity in RA is dependent on the daily dose, total dose, and dosing schedule. Beneficial effects on damage progression are apparent at low doses. These effects may be independent of the symptomatic effect, additive to that of other DMARDs, and may continue well after glucocorticoids are discontinued. Although the potential toxicity is considerable, in practice, it is similar to that of other antirheumatic agents (including NSAIDs).
- © 2007 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.