

Summary
This article discusses the clinician's role in managing osteoporosis, ways to reduce the incidence of fractures, recent studies in postmenopausal women with osteoporosis, an overview of several new treatment options for osteoporosis that target novel pathways, and differences in osteoporosis between men and women, among other things.
- metabolic bone disease
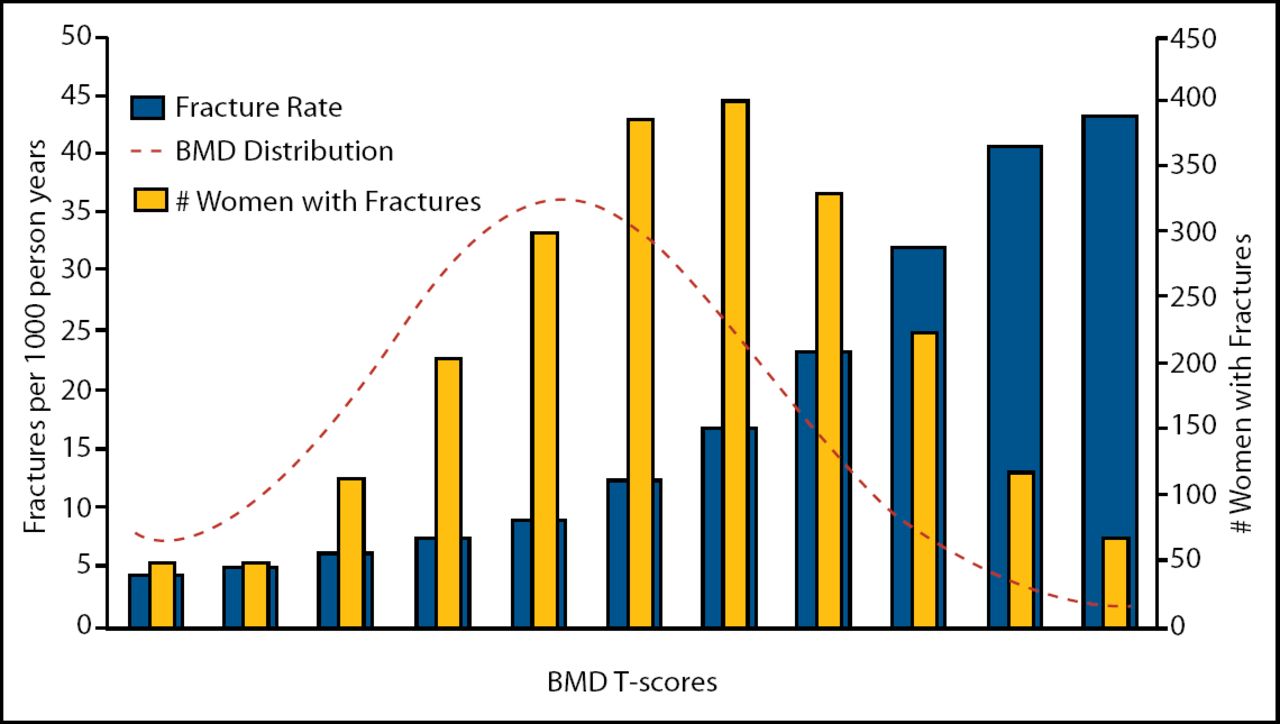
According to Eugene V. McCloskey, MD, University of Sheffield, UK, the aim of the clinician in managing osteoporosis is to reduce the incidence of fractures. The first step in accomplishing this is to accurately identify the patients who are at increased risk. Epidemiologic studies have shown that >50% of all fractures occur in individuals with a bone mineral density (BMD) above the T-score threshold for osteoporosis (Figure 1). Although BMD plays an important role in determining fracture risk, in actuality, the risk is multi-factorial.

Osteoporotic Fracture Rates.
Source: Siris ES et al J Bone Miner Res 2001; 16: Suppl 1, S337.
A WHO Scientific Group has undertaken a series of meta-analyses, based on individual data from prospective population-based studies, to identify clinical risk factors for fracture and to determine their dependence on age, sex, and BMD. These data have allowed the group to not only identify several risk factors (ie, body mass index, prior fracture, parental history of fracture, corticosteroid use, rheumatoid arthritis, smoking, and alcohol intake), but also to examine the interaction among them.
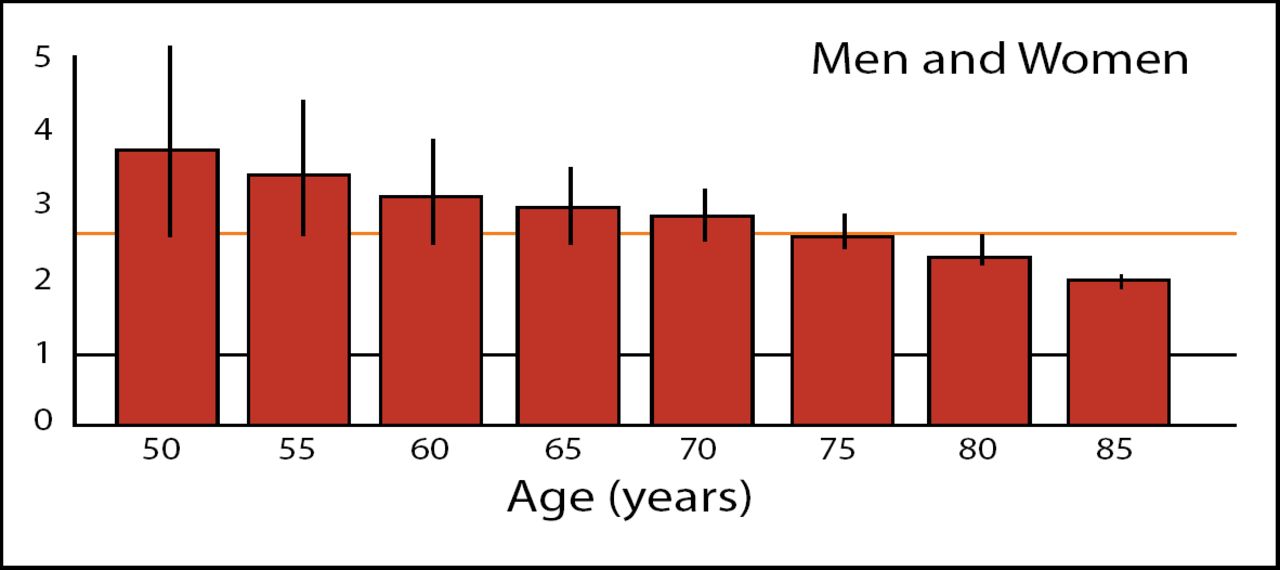
Citing prior studies that have shown a 2.6 fold increase in the risk of hip fracture for every 1 standard deviation decrease in femoral neck BMD [Cummings SR et al. Lancet 1993], Dr. McCloskey noted that when this information is applied across various ages there is an interaction between the two factors such that at age 50, a 1 standard deviation increases the relative risk of hip fracture by 4 fold but at advanced ages the increase is <2.6 (Figure 2). Similar interactions can be seen between BMD and body mass index.

Femoral Neck BMD and Hip Fracture Prediction.
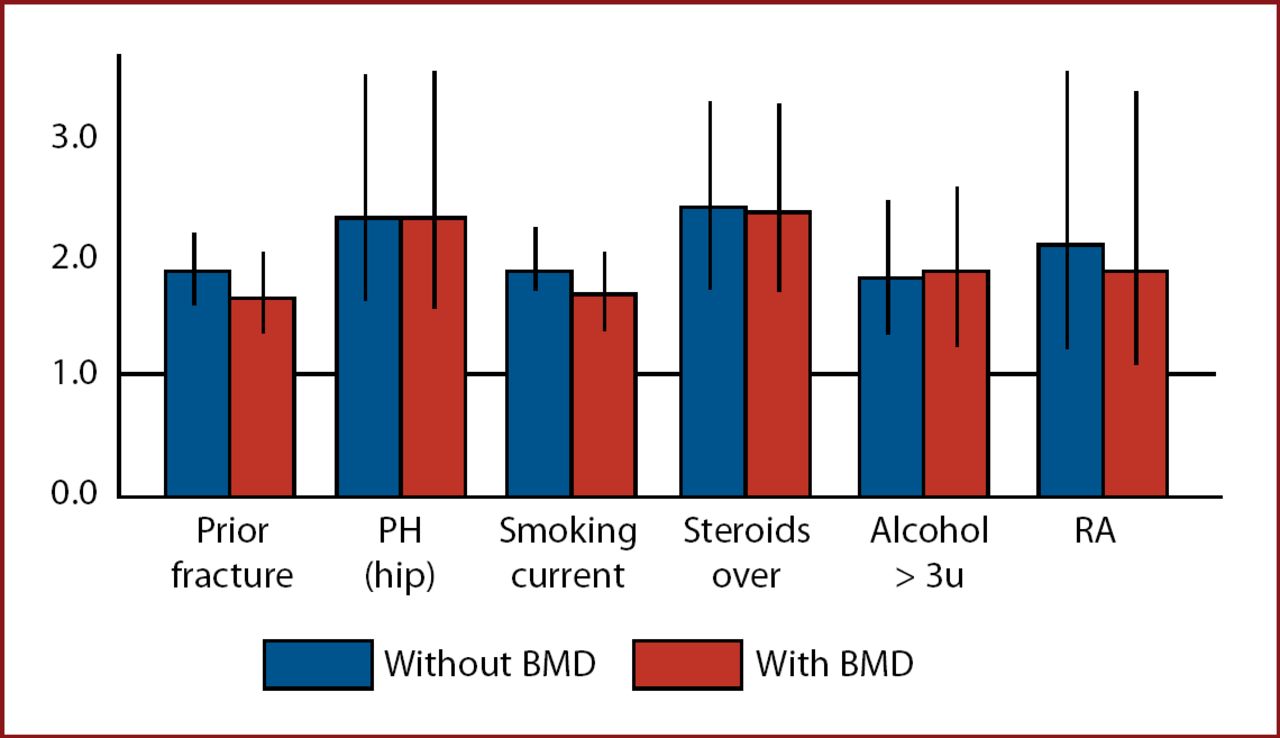
Dr. McCloskey believes that the combined use of these factors provides an assessment of fracture risk that is at least as good as BMD in the prediction of hip and other osteoporotic fractures, and can enhance the performance of BMD as a prognostic tool (Figure 3).

Risk Factors for Hip Fracture in Men and Women.
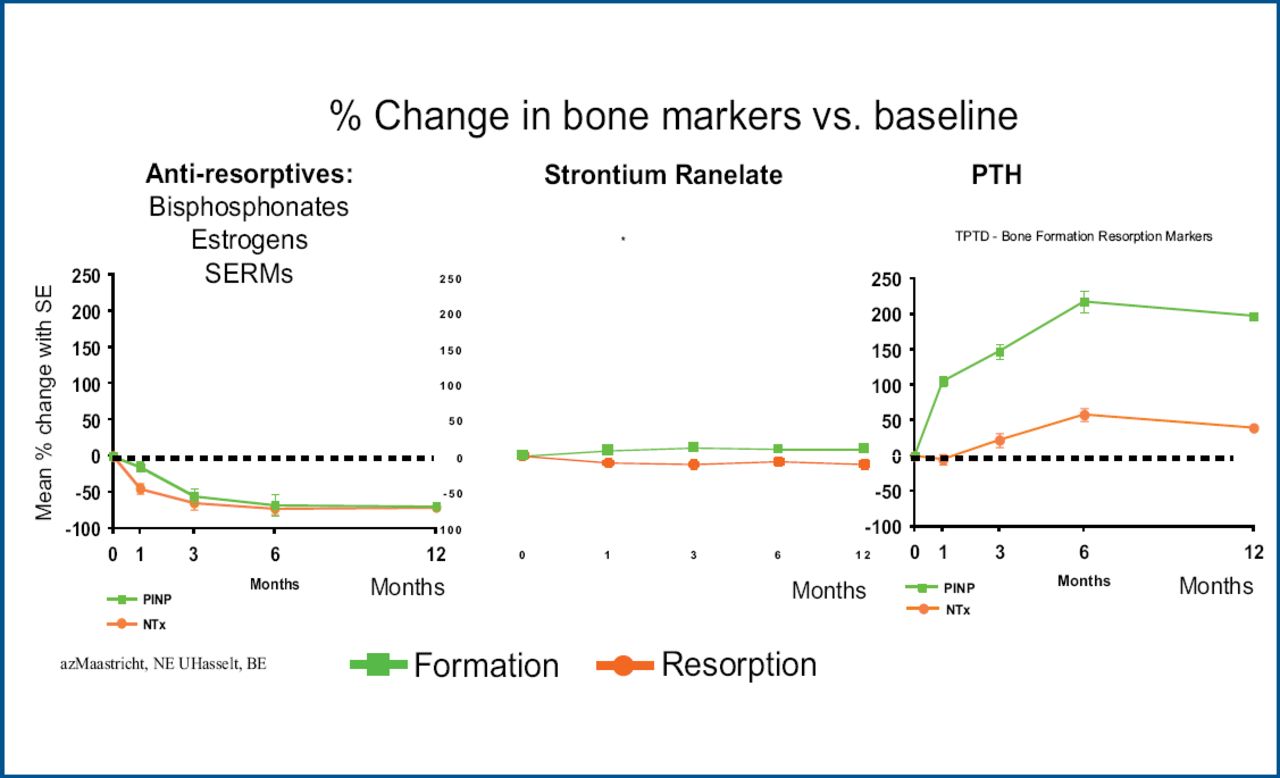
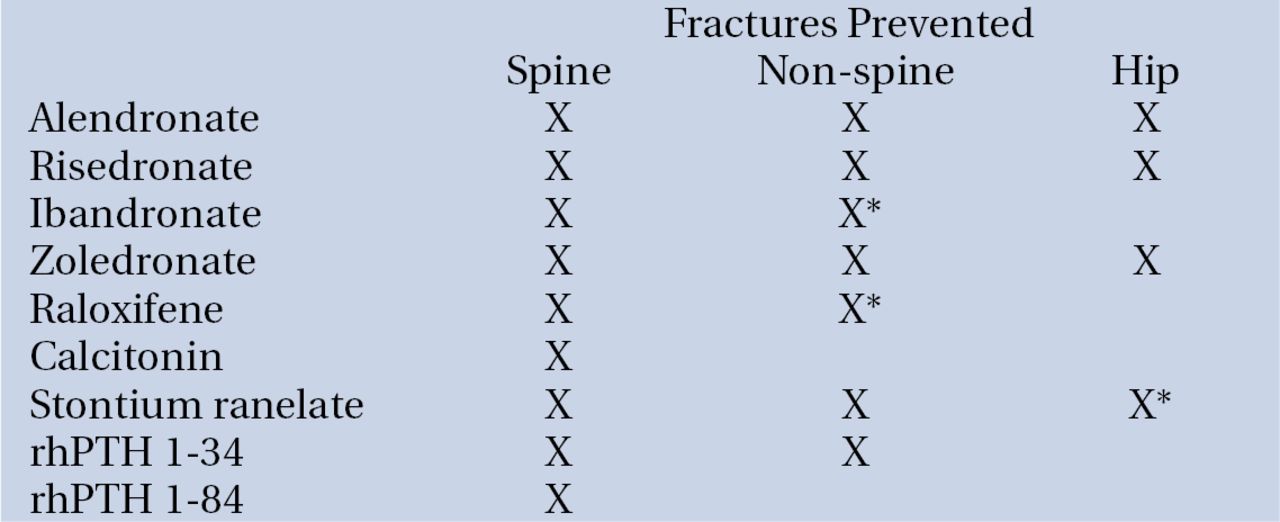
A variety of treatments with proven efficacy for the management of postmenopausal osteoporosis are now available, and each manipulates bone turnover in a different way (Figure 4). There are also differences in their fracture prevention profiles (Figure 5).

Drug Treatment Based on Manipulation of Bone Remodeling.

Anti-Fracture Effects of Drugs in Primary Analysis of RCT's (x) and post-hoc Analyses (x*).
Piet Geusens, MD, University Hospital Maastricht and UHasselt, The Netherlands, presented two examples from recent studies in postmenopausal women with osteoporosis.
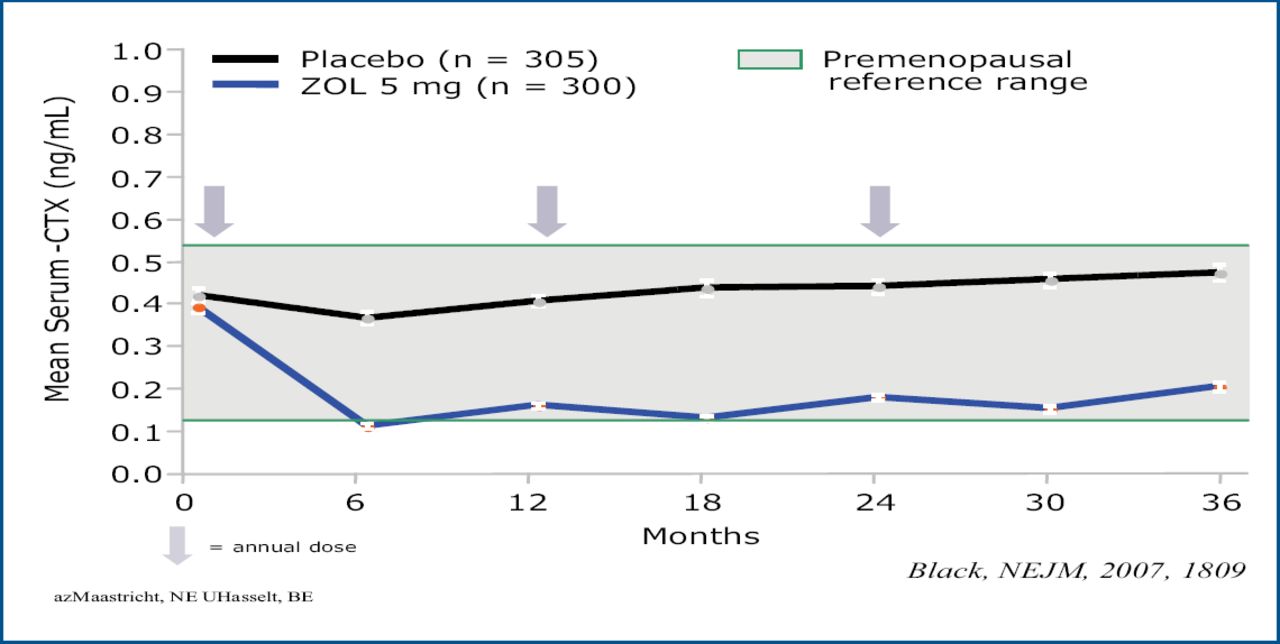
Results from the 3-year HORIZON pivotal fracture trial showed that once yearly treatment with zoledronic acid 5 mg reduced the risk of morphometric vertebral fracture by 70% vs placebo and reduced the risk of hip fracture by 41%. Nonvertebral fractures were reduced by 25% (p<0.001) [Black DM et al. N Engl J Med 2007] (Figure 6).

Zoledronate: HORIZON Pivotal Fracture Trial. Effect of Yearly Infusion on Mean Serum CTX-1.
In the TOP study, which evaluated the effect of recombinant human parathyroid hormone (rhPTH 1–84), there was a 53% reduction in the risk of morphometric vertebral fractures in patients with a prevalent vertebral fracture and 68% reduction in those who did not have fracture, but there was no effect on non-vertebral fractures [Greenspan SL et al. Ann Int Med 2007].
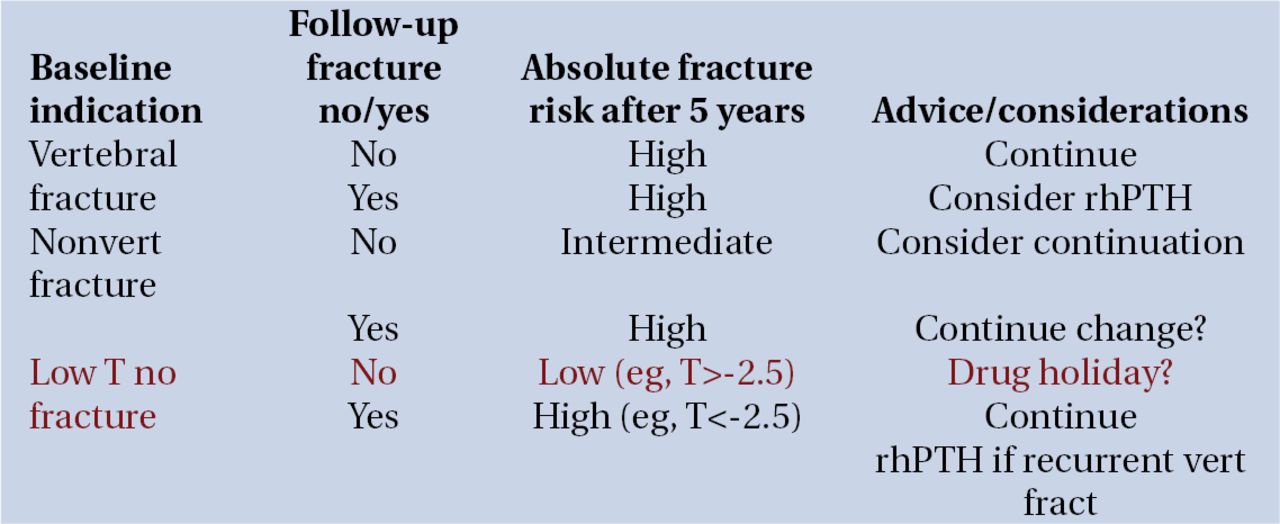
Given the concern over the long-term use of biphosphonates the question of a “drug holiday” after 5 years of treatment has been raised. Studies with risedronate over 7 years [Mellström DD et al. Calcif Tissue Int 2004] and with alendronate over 10 years [Bone HG et al. N Engl J Med 2004] have shown that the risk of fracture remained stable over time. Noncompliance during the first 5 years of treatment increases fracture risk [Gold DT et al. Curr Med Res Opin 2007; Siris ES et al. Mayo Clin Proc 2006] and there are fewer clinical vertebral fractures when treatment is continued past 5 years [Black DM et al. JAMA 2006] with the age-adjusted fracture rate during years 6–10 being similar to that observed during years 1–3 [Bone HG et al. N Engl J Med 2004]. There are a variety of factors to consider when contemplating a drug holiday but Dr. Geusens believes that the strongest is fracture risk. A drug holiday may possible for those with low fracture risk but not for those who continue to be at high risk (Figure 7).

Drug Holiday After 5 Years Treatment with Bisphosphonates? Strategy Examples.
Kenneth Saag, MD, University of Alabama, United States, presented an overview of several new treatment options for osteoporosis that target novel pathways.
RANK ligand is a protein that acts as the primary signal to promote bone removal and in many bone loss conditions it can overwhelm the body's natural defense against bone destruction. Monoclonal technology now allows for the development of inhibitors to RANK ligand. Denosumab is one such inhibitor. Treatment with denosumab for 12 months has been shown to increase BMD 3.0%–6.7% at the lumbar spine (vs 4.6% with alendronate and −0.8% with placebo) and 1.9%–3.6% at the total hip (vs 2.1% with alendronate and −0.6% with placebo [McClung MR et al. N Engl J Med 2006].
Other new approaches in development include inhibitors of sclerostin, an inhibitor of bone formation and cathepsin K, a cysteine protease that plays an essential role in osteoclast function. The objective with cathepsin K inhibition is to block resorption, but to do it at a later disease stage than the biphosphonates where it might be possible to separate the effects on suppression of resorption and suppression of bone formation.
Although this is an exciting time in bone research, Dr. Saag cautioned that we still face many challenges, including potential safety issues with long-term use of biphosphonates. These include severe suppression of bone turnover, acute phase response and renal insufficiency (seen more often with more potent IV biphosphonates), osteonecrosis of the jaw (ONJ), and atrial fibrillation. To date there have been >2000 reports of ONJ predominantly in patients with malignancies who are receiving very high doses of IV biphosphonates. A major problem with ONJ is that the etiology and pathogenesis are poorly characterized. The role of oral and lower dose IV bisphosphonates, in particular, remains unclear. It is not known whether there are independent effects of cancer, how ONJ is related to dental pathology (most reports have followed tooth extraction, root canal, etc), or whether there is a role for the infection that seems to accompany it. More studies are needed to gain a better understanding of the biology and epidemiology of ONJ, particularly in the setting of osteoporosis therapy.
Pilar Peris Bernal, MD, Hospital Clinic, Barcelona, commented on some of the differences in osteoporosis between men and women. Osteoporosis in men is increasingly recognized as a problem in clinical practice. Contrary to what is found with women patients, nearly 50% of men have an underlying secondary cause for bone loss, most frequently, glucocorticosteroid therapy, hypogonadism, and alcoholism. In men with idiopathic osteoporosis, the cause is likely heterogeneous (low levels of IGF-1, increased interleukin 1, decreased β-estradiol, history of delayed puberty, osteoblast dysfunction) [Peris P et al. Br J Rheum 1995]. Thus, the evaluation of osteoporosis in men normally includes laboratory testing to identify correctible causes of bone loss. Data on the efficacy of the typical osteoporosis treatments in the prevention of fractures in men is scarce.
Presenters at EULAR agreed that these and other challenges in osteoporosis call for more head-to-head investigations with fracture outcomes, a clearer understanding of the efficacy, effectiveness, and safety of new agents, and expanded data on alternative administration regimens and routes. There is also a need to better understand the safety of these therapies in special populations, including patients on glucocorticoid therapy, nursing home patients, and patients post-fracture. Ultimately, scientists and clinicians worldwide need to find new ways to translate evidence into practice, effect better patient drug adherence, and continue to improve patient care.

- © 2007 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.