

Summary
This article discusses key issues on therapy and treatment for Churg-Strauss Syndrome, Takayasu Arteritis, and primary angiitis of the central nervous system.
- vasculitis
Churg-Strauss Syndrome
Churg-Strauss syndrome (CSS) is a rare systemic vasculitis that is associated with asthma, eosinophilia, sinusitis, neuropathy, and pulmonary infiltrates and carries a significant risk of morbidity. Michael E. Wechsler, MD, Brigham and Women's Hospital, Boston, Massachusetts, USA, discussed the management of CSS from a pulmonary perspective. Unlike rheumatologists, who view CSS in terms of vasculitis, pulmonary specialists view CSS as an asthma issue that is associated with eosinophilia, vasculitis, +/− ANCA, with flares of asthma or vasculitis.
The 1990 American College of Rheumatology Diagnostic criteria for CSS state that four of the following six criteria are required to positively diagnose CSS (85% sensitive, 99.7% specific): moderate to severe asthma, peripheral blood eosinophilia (>10%), mono- or polyneuropathy, pulmonary infiltrates, paranasal sinus abnormality, and extravascular eosinophils/eosinophilic vasculitis. CSS can be diagnosed without vasculitis, but there must be blood eosinophilia; there should be tissue eosinophilia and asthma with some evidence of extrapulmonary involvement.
Early use of steroids (1 to 2 mg/kg/day for several months) is effective in >90% of CSS patients. Steroids inhibit eosinophil colony growth, cytokine production, and eosinophil survival. However, in addition to the side effects, not all patients initially respond to steroids, very few discontinue treatment when they do respond, and the disease often recurs with steroid withdrawal. Based on clinical experience, the use of steroids alone works best in patients with mild disease and no kidney, gastrointestinal, heart, or central nervous system (CNS) involvement. When steroids alone are unsuccessful, intravenous immunoglobulin, rituximab, anti-IgE, interferon, methotrexate, azathioprine, imatinib, and possibly anti-IL-5 (mepolizumab) can be employed as add-on therapy.
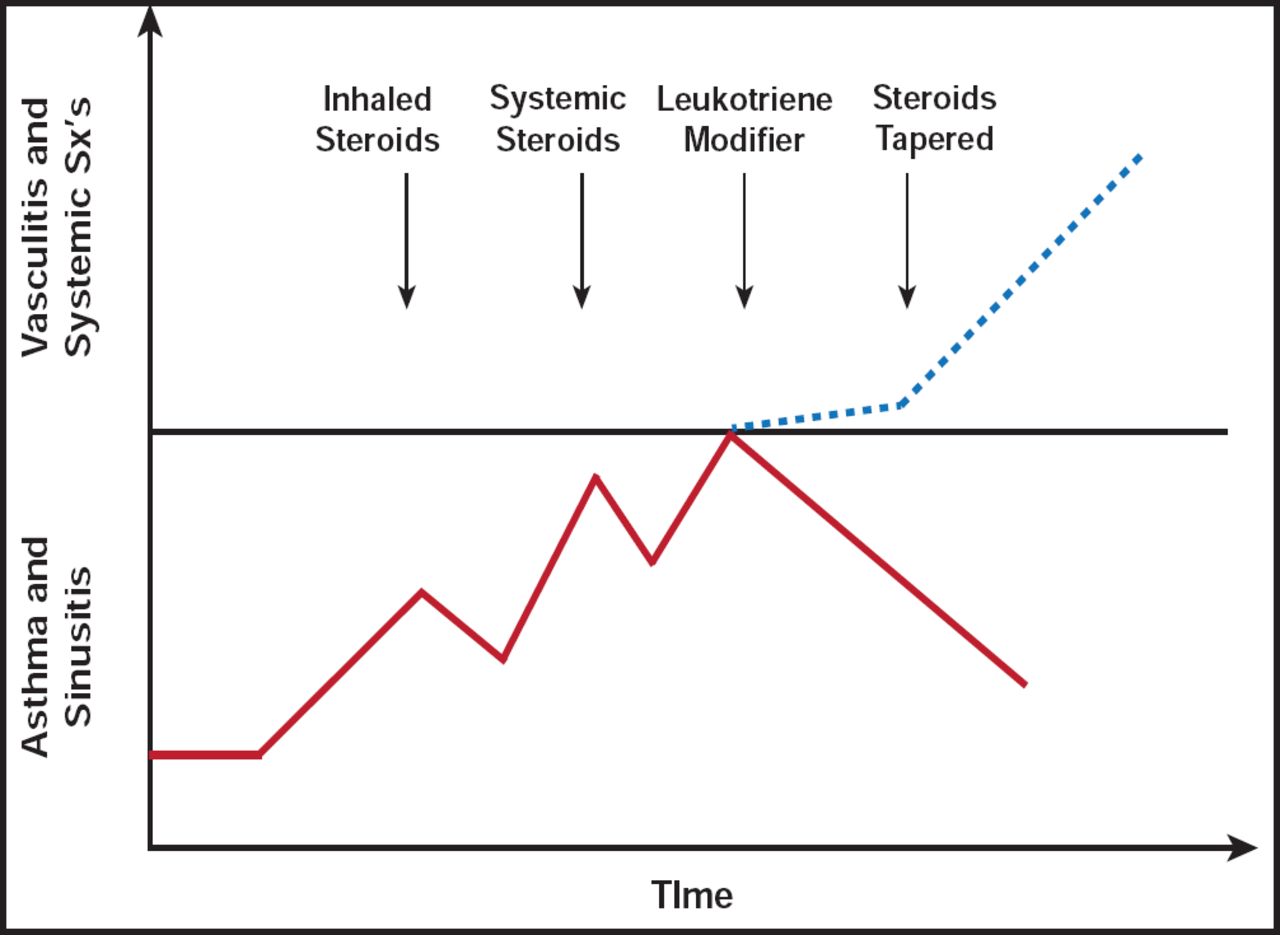
CSS may develop in patients who receive asthma medications and have an underlying eosinophilic disorder that is unmasked by the withdrawal of corticosteroid therapy. Omalizumab (a monoclonal antibody that binds IgE) treatment may unmask CSS due to the weaning of corticosteroids in some asthma patients or may delay corticosteroid treatment, allowing CSS to manifest (Figure 1) [Wechsler ME et al. Chest 2009].

Treatment Strategy.
Reproduced with permission from M. Wechsler, MD.
When treating CSS, it is important to weigh the risks and benefits of all possible therapies. Eosinophilic lung diseases are not as rare as originally assumed. There is a strong need to develop an eosinophilia consortium/network to study CSS and other eosinophilic diseases.
Primary Angiitis of the CNS
Primary angiitis of the CNS (PACNS) is a rare form of angiitis that can be difficult to diagnose and can be confused with reversible cerebral vasoconstriction syndrome (RCVS). Cerebral angiograms have poor specificity in the diagnosis of PACNS; thus, a comprehensive approach is warranted to make the diagnosis. Rula Hajj-Ali, MD, Cleveland Clinic Foundation, Cleveland, Ohio, USA, discussed ways to recognize and differentiate PACNS from other CNS diseases.
The diagnostic criteria for PACNS include: 1) the presence of an unexplained neurological deficit after thorough clinical and laboratory evaluation; 2) documentation by cerebral angiography and/or tissue examination of an arteritic process within the CNS; and 3) no evidence of a systemic vasculitis or any other condition to which the angiographic or pathological features could be secondary. Common symptoms include headaches (63% of patients) that are indolently progressive and not severe enough to warrant emergency evaluation; encephalopathy due to diffuse cortical dysfunction; persistent neurological deficits (40% of patients); and nonspecific, insidious symptoms.
Typical cerebrospinal fluid findings include aseptic meningitis. Abnormal magnetic resonance imaging findings, in almost all patients, are seen in the subcortical white matter, deep gray matter, deep white matter, and cerebral cortex. Infarcts may be seen in approximately 50% of cases.
Angiography findings can include stenosis, ectasia, and beading in multiple vessels. Angiographic findings of PACNS are often associated with other specific pathological diagnoses (eg, premature intracranial atherosclerosis, fibromuscular dysplasia, radiation vasculopathy, Moyamoya disease, and RCVS) and thus are not a specific modality in the diagnosis of CNS vasculitis. A brain biopsy is often required to secure the diagnosis of PACNS or to rule out other conditions.
RCVS, often confused with PACNS, is notable as having multiple areas of stenosis, followed by normal caliber or distended arteries; normal or near-normal cerebrospinal fluid analysis; and severe, acute, often recurrent thunderclap headache, with or without additional neurological signs or symptoms. Reversibility of the cerebrovascular abnormalities is essential to confirm the diagnosis of RCVS and occurs in approximately 60 days.
A comprehensive approach is essential when entertaining the diagnosis of PACNS. Findings of multiple areas of stenosis and dilatation on cerebral angiogram are not specific for the diagnosis of PACNS. Clinicians should be aware of RCVS, since it is a common mimic of PACNS.
Takayasu Arteritis
Takayasu Arteritis (TAK) is a form of large-vessel granulomatous vasculitis with massive intimal fibrosis and vascular narrowing, often affecting young or middle-aged women. It mainly affects the aorta and its branches, as well as the pulmonary arteries. Peter A. Merkel, MD, Boston University School of Medicine, Boston, Massachusetts, USA, discussed the role of different imaging techniques in TAK, how useful these techniques are in assessing disease, and treatment options.
Diagnostic imaging is essential for diagnosis and management of TAK and may be performed via catheter-based angiography, MR angiography, CT angiography, ultrasonography, or PET/CT. The goals of imaging studies are to obtain an accurate assessment of arterial anatomy, which includes morphological assessment of the luminal artery narrowing, evidence of stenosis or occlusion, aneurysms, collateral flow, and revascularization. Silent disease is common (initially found lesions may be old or inactive). It is important to fully image the aorta and main first- and second-order branches to determine the full extent of the disease. Progression of lesions is common, even after inflammatory disease is controlled. Healing may involve fibrosis, scarring, and more arterial narrowing and symptoms. Collaterals may form to counter the physiological impact of stenosis.
Dr. Merkel recommends caution when interpreting MR/CT/PET findings for TAK. The specificity of arterial wall enhancement is not known; surgical specimens do not always show inflammation, and there is relatively little data for PET studies. The predictive value of these lesions is not clear, in that many such findings never lead to arterial stenosis, even in untreated patients, and patients may go years with “enhancement” and no progression. Despite these caveats, Dr. Merkel feels that catheter-based angiography, MR angiography, and CT angiography are good diagnostic tools for TAK. For monitoring disease progression and activity, MR angiography, CT angiography, and ultrasonography are best. PET is still exploratory but may be a good complementary tool. Conventional angiography is advantageous, as it allows for direct blood pressure measurements and simultaneous intervention with angioplasty and/or stents if necessary.
Treatment for TAK may take the form of medical therapy (glucocorticoids, immunosuppressive drugs, biologic agents, and aspirin/antiplatelet agents) or revascularization (surgery or stents). Other considerations must include careful treatment and monitoring of blood pressure, lipid control, and lifestyle modification (exercise and diet).
- © 2011 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.