

Summary
Pamela S. Douglas, MD, President of the American College of Cardiology, and Chief, Cardiovascular Medicine, Duke University, launched the 55th Annual Scientific Session of the American College of Cardiology with a Presidential Address titled “Improving Imaging: Our Professional Imperative.”
- imaging
- cardiac imaging (radiology)
Pamela S. Douglas, MD, President of the American College of Cardiology, and Chief, Cardiovascular Medicine, Duke University, launched the 55th Annual Scientific Session of the American College of Cardiology with a Presidential Address titled “Improving Imaging: Our Professional Imperative.”

“New diagnostic tools and creative treatments have sparked an exciting evolution in medicine,” said Dr. Douglas. “And while this would seem to be a positive change, sometimes we adopt these new tools with not enough thought to ensuring quality.”
Cardiovascular imaging, she said, is a case in point. “If imaging were a drug, regulatory approval would be denied,” she said, calling for more and better research, standards, and guidelines in CV imaging.
Medical imaging joined such fundamental innovations as anesthesia and antibiotics when the New England Journal of Medicine cited the top 11 medical developments of the past millennium. Two years after that announcement the landmark study “Physician's Views of the Relative Importance of 30 Medical Innovations” (Fuchs VR et al, Health Affairs Vol. 20, #5, Sept/Oct 2001) reported on a survey of U.S. internists that identified MR/CT as the single most important innovation of the last quarter-century.
As imaging has moved to the forefront of innovation, cardiology has served as a fertile creative platform and testing ground for many of imaging's advances, and continues to do so. These advances have certainly enhanced detection and diagnosis and enabled interventions of unparalleled success. A few of the more intriguing areas of research and treatment include:
Cardiac magnetic resonance imaging (CMI) has several advantages over echocardiography, including fewer artifacts and unlimited acquisition windows. CMI is noninvasive, carries no radiation risks, uses benign contrast agents, and offers comprehensive information from a single examination. To obtain similar information currently requires a complicated and time-consuming combination of diagnostic tests. Software development has made, real-time imaging possible and has decreased data acquisition time.
Contrast-enhanced magnetic resonance angiography (MRA) with “bolus chase” is a technique achieved by administrating a contrast bolus into a peripheral vein and then “chasing” the bolus on its voyage through the vasculature of the abdomen, pelvis, and lower extremities. Bolus-chase MRA has allowed for quick and reproducible angiography of the abdominal aorta, pelvis, and lower extremities in evaluating peripheral arterial disease. MRA has also demonstrated promise in other vascular imaging, notably in post-procedure evaluation of aortic endovascular stent grafts.
Multidetector computed tomographic (MDCT) scanning has emerged as a complementary technique to echo, particularly in evaluating congenital heart disease. MDCT very accurately images the aorta, right ventricle, and pulmonary artery. The newer MDCT scanners have augmented the ability of CT angiography to identify pulmonary embolism. MDCT is an example of an imaging innovation that mitigates (or removes) traditional sources of confusion in earlier forms of imaging, particularly in the lungs (e.g., pulmonary veins, non-specific densities, lymphatics, etc.)
Computed tomographic angiography (CTA) has shown potential in planning interventional vascular therapy. With a very large portfolio of images and techniques of “automated vessel extraction” both quantitative and visual assessments can be achieved.
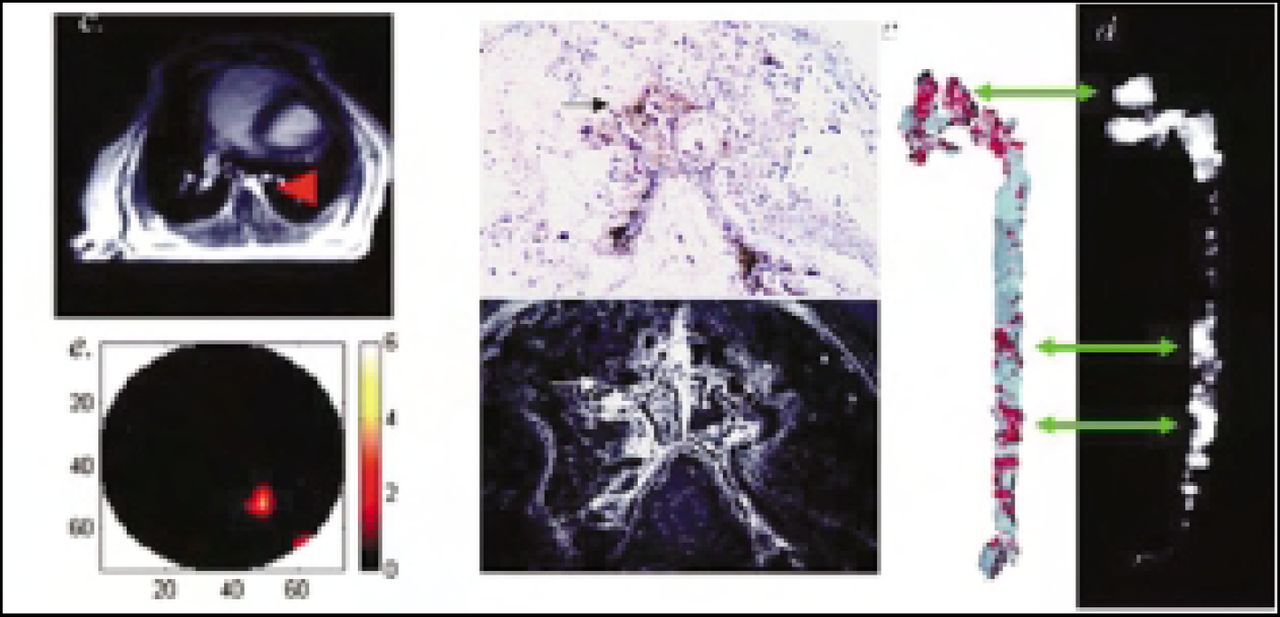
Cardiovascular molecular imaging (CMI) is implemented by contrast-tagged molecular agents (either organic compounds or synthetic nanoparticles) which are injected and subsequently bind to target molecules in the heart and vasculature. (This technique has been experimentally demonstrated in laboratory animals by “lighting up “ fibrin as a marker for plaque rupture, as well as detecting angiogenesis of vessels supporting plaques.) Contrast-tagged molecular agents can serve to visualize pathological states or activities, as drug-delivery vehicles, or both.

Popular magazines, including Time and U.S. News and World Report, have reported “glimpes into the future” in recent issues that characterize cardiac imaging using varieties and combinations of the above technologies. A “heart test” in the near future might utilize a “fusion application” that will generate a personalized profile revealing ventricular volumes and function, valvular structure, function, and dynamics, and coronary artery anatomy with luminal images of startling resolution. From the information obtained, a patient can be risk-stratified—educated appropriately, placed on an evidence-based plan, and treated if therapy is indicated. And, indeed, the technology to achieve all of this is, for the most part, in place or moving quickly toward reality.
But as exciting as these imaging alternatives are, clinicians are often divided on appropriate applications, benefits, and safety. This point was indirectly emphasized by the many imaging-related presentations at ACC 2006, many of which discussed a spectrum of applications for a variety of imaging strategies, from conventional tools used in new ways to various combinations of conventional and emerging techniques. A key concern through all of this—and the focus of Dr. Douglas's Presidential Address—is that bioengineering and technological progress in CV imaging has generally outpaced research and randomized clinical trial data. State-of-the-science assessments and meta-analyses have been confounded by this schism between accelerated progress vs. data in which even recently published reports lag behind available technology.
As one expert observer has noted, medical imaging is a moving target. With that in mind, “We must demand better imaging research, develop pragmatic research methods, create imaging standards for trials, define imaging quality and outcomes, and improve imaging effectiveness and efficacy in practice,” Dr. Douglas said.
In citing rapid growth of technologies, widespread applications, inconsistent use, few regulatory controls, and a paucity of evidence for outcomes, Dr. Douglas pointed to a lack of consensus on the definition of quality as a prime reason why the cardiovascular community must take the lead on quality in imaging. “Improving quality cardiovascular imaging is a professional imperative,” she said.
- © 2006 MD Conference Express
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.