

Summary
This article discusses new insights on the diabetic eye, assessing and managing ocular complications of diabetes, as well as diabetic kidney disease.
- Retinal Diseases
- Diabetes & Kidney Disease Diabetes Mellitus
- Renal Disease
- Retinal Diseases
- Diabetes & Kidney Disease
- Endocrinology
- Diabetes & Metabolic Syndrome
- Diabetes Mellitus
- Renal Disease
NEW INSIGHTS ON THE DIABETIC EYE
According to Jennifer K. Sun, MD, MPH, Joslin Diabetes Center, Boston, Massachusetts, USA, the 7-standard field color fundus photography protocol established by the Early Treatment Diabetic Retinopathy Study [ETDRS], which captures 90° of the posterior retina and 30% of the entire retinal surface, is the gold standard currently used to evaluate the eye complications of diabetes [Garg S, Davis RM Clin Diabetes 2009]. This procedure requires pharmacologic pupil dilation and a skilled retinal photographer. However, a less extensive evaluation can be performed with nonmydriatic ultrawide field imaging (UWFI), which can capture up to 200° and 82% of the entire retinal surface in a single image [Soliman AZ et al. Semin Ophthalmol 2012] and requires no pupil dilation.
Telemedicine is an important element of screening for diabetic retinopathy. However, the official standard of the American Telemedicine Association (ATA) for validating retinal images is the ETDRS protocol [ATA Telehealth Practice Recommendations for Diabetic Retinopathy 2011]. As ETDRS requires a skilled operator, however, it is not always accessible to remote clinics.
Evidence suggests that the wider range of UWFI can capture more cases of diabetic retinopathy than ETDRS, as well as detect more hemorrhages and intraretinal abnormalities [Silva PS et al. Ophthalmology 2013]. One study suggests that compared with ETDRS, UWFI could identify more severe retinopathy, reduce the rate of ungradable diabetic retinopathy by 71%, and reduce the time to image evaluation [Silva PS et al. Diabetes Care 2014]. According to Dr. Sun, UWFI may become a new standard in clinical, research, and teleophthalmology settings if these findings are confirmed in trials across all severity groups.
MANAGING OCULAR COMPLICATIONS
Lloyd Paul Aiello, MD, PhD, Joslin Diabetes Center, Boston, Massachusetts, USA, spoke about assessing and managing ocular complications of diabetes. He emphasized that proliferative diabetic retinopathy is the leading cause of severe visual loss in people with diabetes and that severe retinopathy can exist with good vision. Therefore, appropriate care mandates that clinicians be proactive, as patients with diabetic eye complications often remain unaware of their eye disease [Huang OS et al. Ann Acad Med Singapore 2009]. As well, lack of patient awareness is a major factor in nonadherence to eye care guidelines and poor visual outcomes [Schoenfeld ER et al. Ophthalmology 2001].
According to guidelines published by the American Diabetes Association (ADA), adults with type 1 diabetes mellitus should undergo an initial ophthalmic exam within 5 years of onset or shortly after the diagnosis of type 2 diabetes (T2DM) [ADA. Diabetes Care 2014]. Dr. Aiello reinforced 6 elements composing state-of-the-art diabetes care: (1) identification; (2) lifelong evaluation and education; (3) optimization of systemic factors, such as blood glucose, blood pressure (BP), and lipids; (4) identification of complications; (5) timely and appropriate intervention; and (6) novel therapies and treatment approaches.
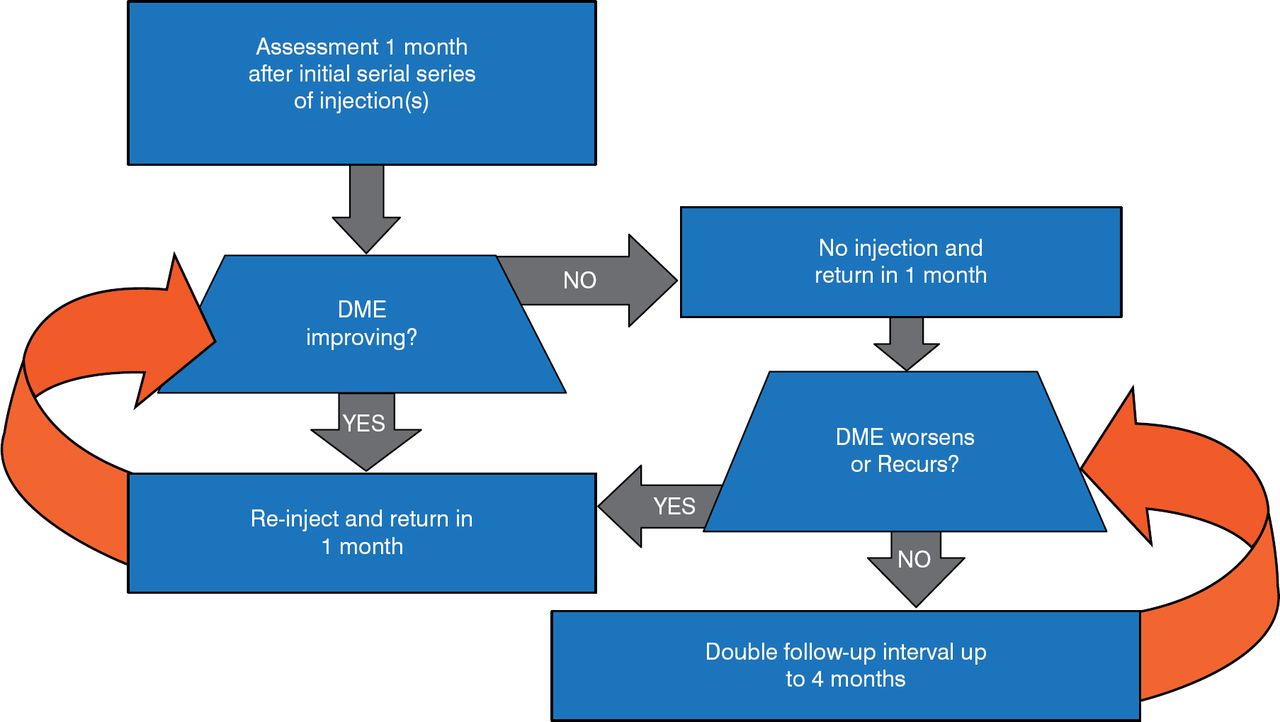
Diabetic macular edema (DME), caused by retinal microvascular changes, is an important cause of vision loss. An injection of intravitreal ranibizumab, followed by prompt (within 1 week of initial injection) or deferred laser photocoagulation, was more effective through ≥ 1 year compared with prompt laser alone for treating central DME [Diabetic Retinopathy Clinical Research Network et al. Ophthalmology 2010]. An algorithm for the treatment and follow-up of center-involved DME with antivascular endothelial growth factors is provided in Figure 1.

Treatment Scheme for Center-Involved DME With Anti-VEGF Agents
DME = diabetic macular edema; VEGF = vascular endothelial growth factors.
DIABETIC KIDNEY DISEASE
Diabetes is the leading cause of end-stage renal disease (ESRD). Ian H. de Boer, MD, MS, University of Washington, Seattle, Washington, USA, stated that diabetic kidney disease (DKD) has not decreased in people with diabetes despite an increased use of medications to control BP and glucose levels [de Boer IH et al. JAMA 2011]. The biomarker cystatin C, alone or in combination with creatinine, improves the estimation of glomerular filtration rate (eGFR) [Shlipak MG et al. Am J Kidney Dis 2013; Inker LA et al. N Engl J Med 2012] and the classification of cardiovascular risk [Shlipak MG et al. N Engl J Med 2013]. However, cystatin C may not significantly improve the tracking of eGFR [de Boer IH et al. J Am Soc Nephrol 2014.
Strategies to reduce the progression of DKD and reduce cardiovascular risk focus on 6 targets: BP, glycemia, albuminuria, weight loss and exercise, nephrotoxins, and novel therapies. Dr. de Boer reviewed various published BP targets (Table 1) and data suggesting that while intensive BP control had no benefit on kidney disease progression, it may benefit patients with baseline proteinuria [Appel LJ et al. N Engl J Med 2010].
Blood Pressure Targets Recommended by Professional Societies
Although calcium channel blockers (CCBs), angiotensin-receptor blockers (ARBs), and ACE inhibitors all effectively lower BP, there are differences among them. ACE inhibitors have demonstrated greater cardiovascular benefit than that of ARBs (Cheng J et al. JAMA Intern Med 2014). Among patients with DKD and T2DM, ARBs have demonstrated more renal benefit than have CCBs (Lewis EJ et al. N Engl J Med 2001]. However, the use of an ARB plus an ACE inhibitor is likely to provide no additional benefit and may increase the risks of hypotension, hyperkalemia, and acute kidney injury [Hsu TW et al. JAMA Intern Med 2014; Hou FF et al. N Engl J Med 2006]. There are also data suggesting the benefit of taking at least 1 BP medication at night to prevent clinical cardiovascular events [Hermida RC et al. J Am Soc Nephrol 2011; Hermida RC et al. Diabetes Care 2011].
Article Notes
-
↵* On September 4, 2014, the article author was changed from Mary Mosley to Jill Shuman.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.