

Summary
According to substudy of the Action to Control Cardiovascular Risk in Diabetes [ACCORD; NCT00000620] trial, intensive glycemic control and combination fenofibrate + simvastatin therapy reduce the rate of diabetic retinopathy progression.
- Retinal Diseases
- Diabetes Mellitus
- Lipid Disorders
- Prevention & Screening
- Diabetes & Endocrinology Clinical Trials
- Hypertensive Disease
According to substudy of the Action to Control Cardiovascular Risk in Diabetes (ACCORD; NCT00000620) trial, intensive glycemic control and combination fenofibrate + simvastatin therapy reduce the rate of diabetic retinopathy progression. Emily Y. Chew, MD, National Eye Institute, Bethesda, MD, presented findings from a substudy of ACCORD.
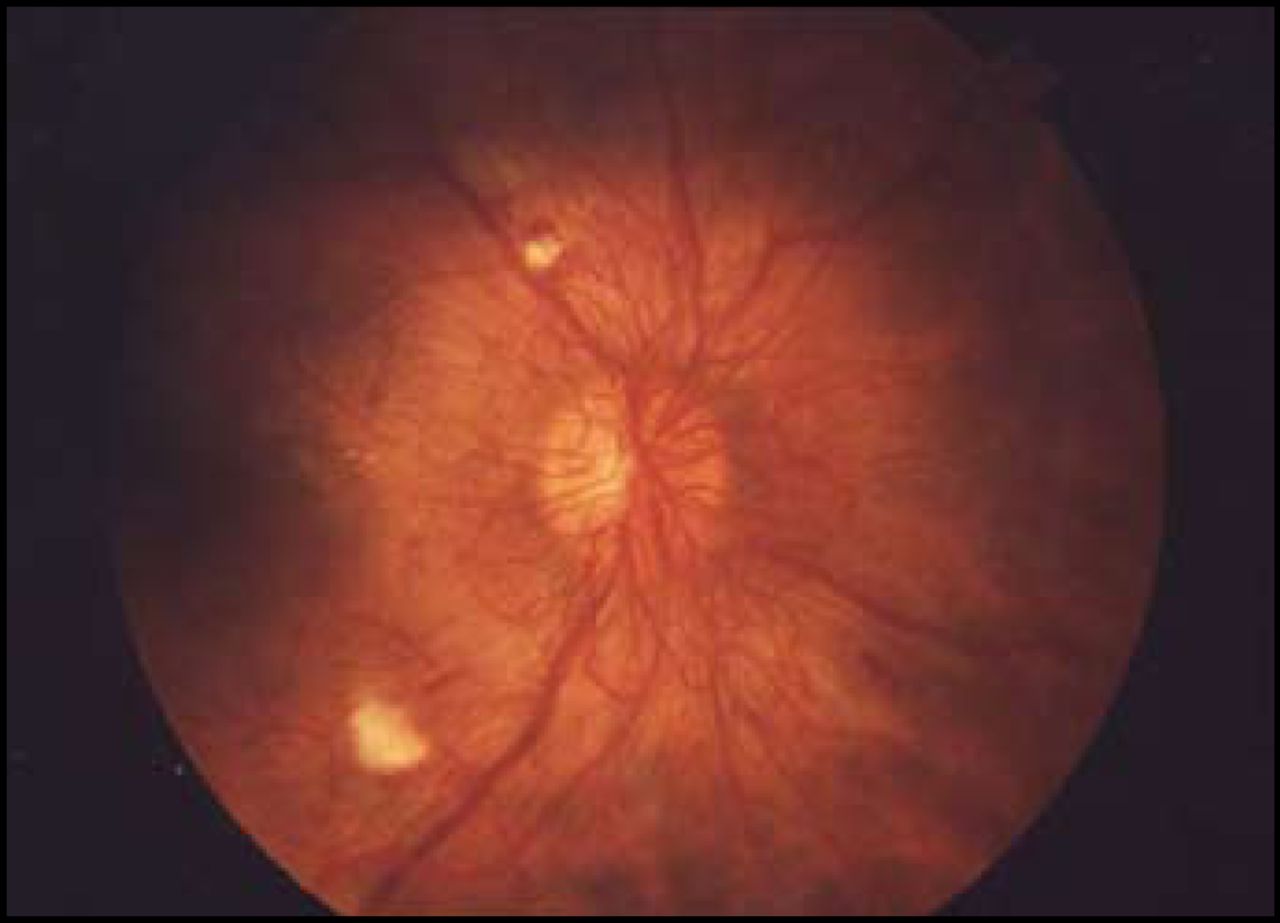
The ACCORD eye study included a comprehensive eye evaluation that included visual acuity measurement, fundus photography of 7 standard stereoscopic fields (Figure 1), and central grading of the fundus photography using the Early Treatment Diabetic Retinopathy Study (ETDRS) classification scale of diabetic retinopathy. These exams were administered at baseline and at Year 4. The objective of this study was to determine whether intensive glycemic control, intensive blood pressure control, or combination (fenofibrate + simvastatin) therapy for dyslipidemia would affect the progression of diabetic retinopathy in patients with type 2 diabetes mellitus (T2DM). ACCORD participants were excluded from participation in this substudy if they had previous laser photocoagulation, vitrectomy, or inability to progress 3 steps on the ETDRS scale of diabetic retinopathy severity.

Diabetic Retinopathy.
Reproduced with permission from E. Chew, MD.
The primary outcome was progression of retinopathy, defined as the progression of diabetic retinopathy of ≥3 levels on the EDTRS scale, assessed on fundus photographs at 4 years compared with baseline; photocoagulation; or vitrectomy during follow-up. Patients who participated in the ACCORD eye study who had both baseline and follow-up visits (n=2856) were included in the final data analysis. Of the 3472 patients who were seen for baseline visits, 616 were missing at follow-up. The mean HbA1C was 8.2%, the mean high-density lipoprotein cholesterol was 41.9 mg/dL, the mean low-density lipoprotein cholesterol was 100.7 mg/dL, and mean triglyceride level was 195.1 mg/dL. The mean systolic blood pressure (BP) in this group was 134.5 mm Hg, and the mean diastolic BP was 74.9 mm Hg.
A total of 253 patients had progression of retinopathy (8.9%) at 4 years, of which 7.3% was in the intensive therapy group (n=104/1429) and 10.4% was in the standard therapy group (n=149/1427). Progression of retinopathy was more frequent among patients who received standard glycemic therapy versus intensive therapy (OR, 0.67; 95% CI, 0.51 to 0.87; p=0.003). Patients who received combination lipid therapy also had less incidence of retinopathy progression compared with placebo (OR, 0.60; 95% CI, 0.42 to 0.87; p=0.006).
Intensive glycemic and combination lipid therapy significantly reduced the incidence of progressive retinopathy at 4 years. These effects were consistent across subgroups. Intensive BP control to 120 mm Hg did not appear to influence the progression of retinopathy. No significant interactions were found with regard to any of the prespecified subgroups.
- © 2010 MD Conference Express
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.