

Summary
In patients with anterior ST segment elevation myocardial infarction who are treated by primary percutaneous coronary intervention (PCI), adjunct treatment with intracoronary (IC) eptifibatide did not improve the primary endpoint of post-PCI epicardial flow compared with IC tirofiban.
- interventional techniques & devices
- myocardial infarction clinical trials
In patients with anterior ST segment elevation myocardial infarction (STEMI) who are treated by primary percutaneous coronary intervention (PCI), adjunct treatment with intracoronary (IC) eptifibatide did not improve the primary endpoint of post-PCI epicardial flow compared with IC tirofiban. There was, however, improvement in some secondary endpoints with IC eptifibatide including better myocardial reperfusion, reduction of in-hospital recurrent ischemia, greater ST segment resolution, and more preservation of systolic function with less TIMI minor bleeding compared with IC tirofiban.
When given systemically, platelet glycoprotein IIb/IIIa inhibitors enhance the benefits of primary PCI by improving microcirculation and tissue perfusion and reducing major adverse cardiac events (MACE) [Montalescot G et al. N Engl J Med 2001; Zeymer U. Expert Opin Pharmacother 2007; van't Hof AW & Valgimigli M. Drugs 2009]. Their use in selected patients is supported in the ACC/AHA 2009 STEMI/PCI Guideline Focused Update [J Am Coll Cardiol 2009] and the ESC/EACTS Guidelines on Myocardial Revascularization [Eur Heart J 2010].
IC GP IIb/IIIa inhibitors result in high local drug concentrations and may be more effective than a standard intravenous (IV) bolus in the dissolution of thrombi and micro emboli and thus may lead to improved myocardial microcirculation and reduced no reflow and infarct size with a possible decrease in adverse systemic effects (bleeding, thrombocytopenia) [Srinivasan M & Prasad A. J Invasive Cardiol 2009].
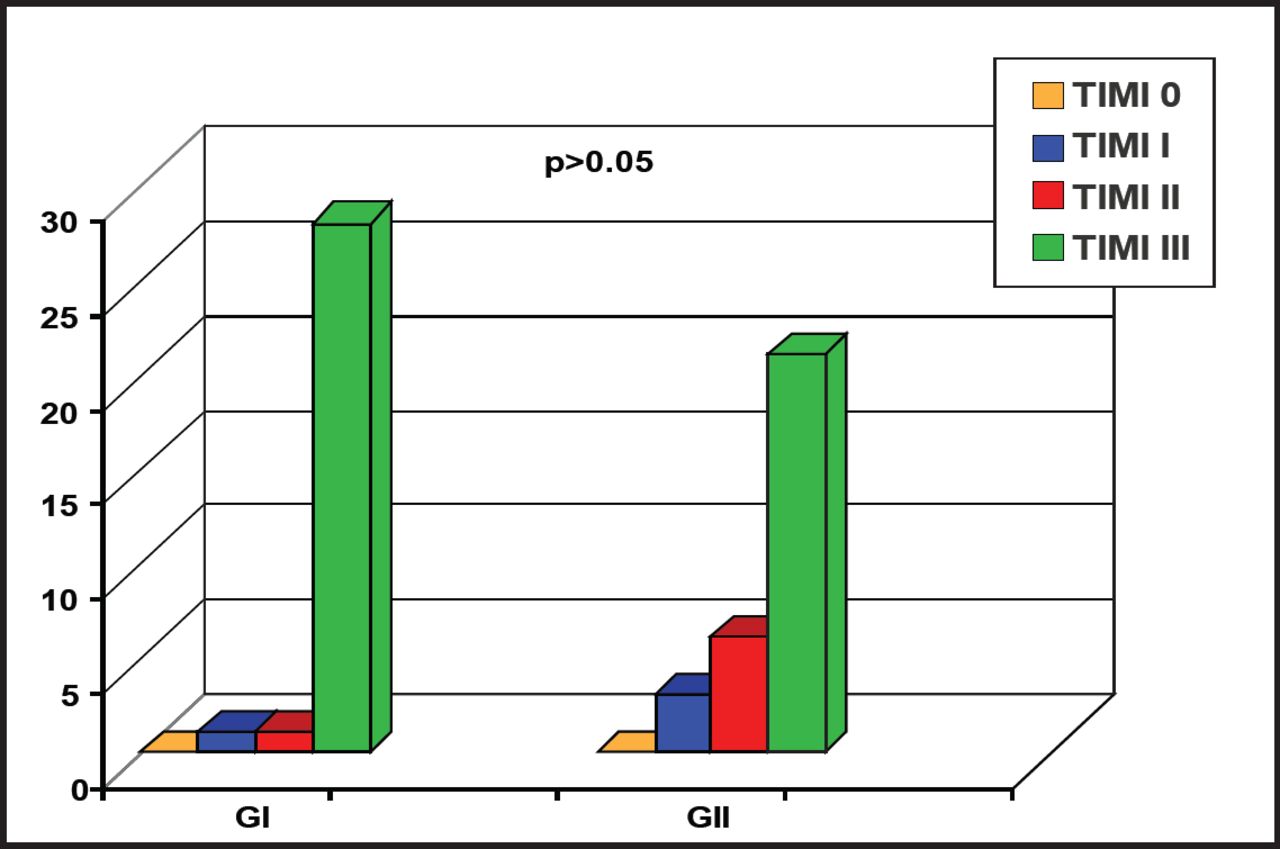
In the study presented by Tamer Abu Arab, MD, Ain Shams University, Cairo, Egypt, 60 patients (mean age 55 years; mostly men) with anterior STEMI undergoing primary PCI were randomized to either two IC boluses of eptifibatide (180 mcg/kg each) just after passage of the wire or first balloon inflation followed by continuous infusion of 2 μg/kg/min for 12 to 24 hours following the primary PCI or a double IC bolus dose of tirofiban (25 μg/kg) just after passage of the wire or first balloon inflation followed by continuous infusion of 0.15 μg/kg/min for 12 to 24 hours following the primary PCI. The two groups were well-matched for baseline clinical, demographic, angiographic and ECG characteristics. All patients received standard dual antiplatelet therapy and heparin (300 mg ASA, 600 mg clopidogrel, and 70 IU/kg unfractionated heparin in the cath lab). The primary end point was achievement of TIMI 3 epicardial flow and at least myocardial blush grade (MBG) 2 or 3 as a measure of successful myocardial (tissue) reperfusion.
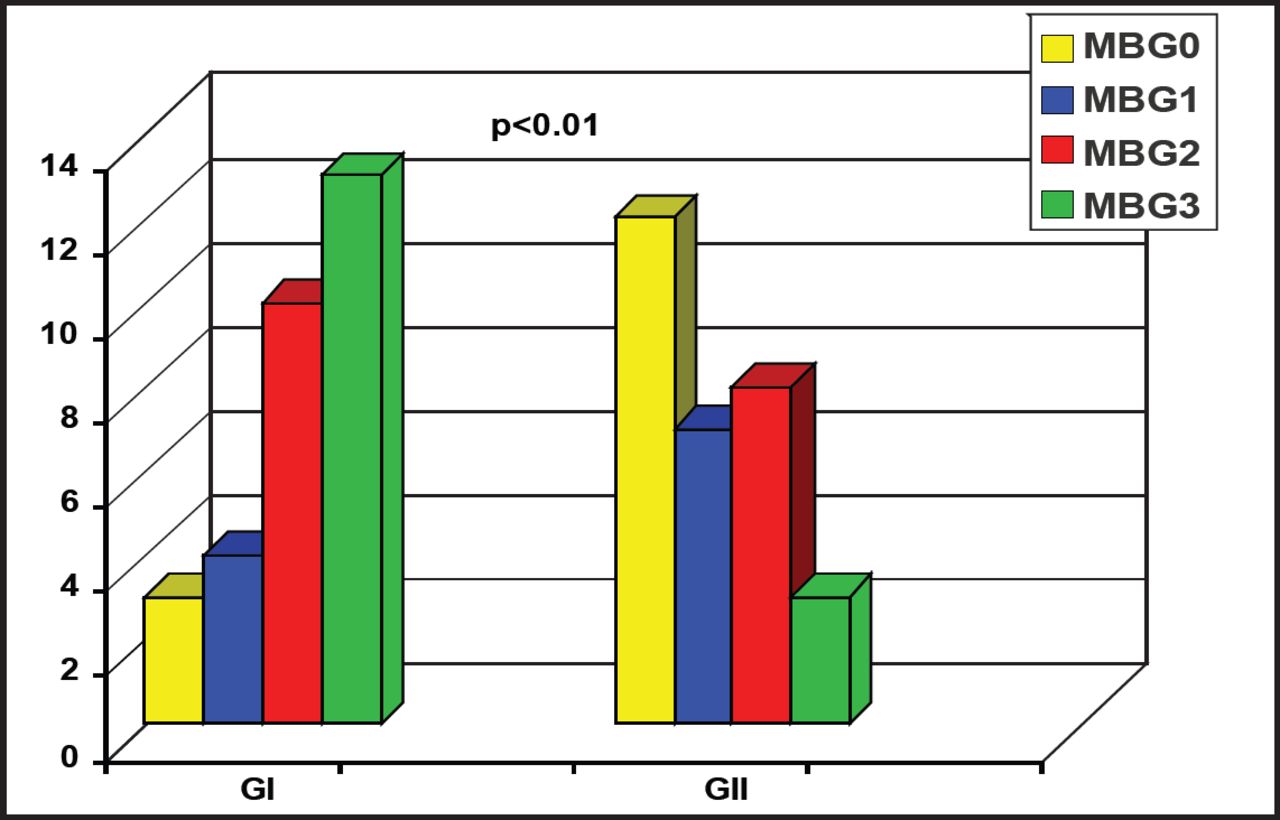
The difference in TIMI 3 flow for the two groups was not significantly different (Figure 1). However, significantly (p=0.005) more patients in the eptifibatide group (76.6%) had MBG grade 2 or 3 versus the tirofiban group (36.6%; Figure 2). There was no significant difference in the rate of in-hospital MACE between groups with one death (3.3%) in each group. None of the patients in the eptifibatide group had recurrent ischemia versus 16.7% of patients treated with tirofiban (p.0.05). Successful ST segment resolution (70.9 % ± 11.3 vs 59.7 % ± 9) and systolic function preservation (ejection fraction of 46.6 ± 5.5 vs 39.9 ± 6) were significantly better in eptifibatide group (p<0.01). TIMI major bleeding was not different between the two groups, however TIMI minor bleeding occurred in 33.3% of tirofiban patients versus no patients in the eptifibatide group (p<0.01).

Primary Endpoint.
Reproduced with permission from TA Arab, MD.

Post PCI MBG Among Study Groups.
Reproduced with permission from TA Arab, MD.
Although the primary endpoint in this trial was not met, favorable trends in secondary endpoints suggest that IC eptifibatide may be beneficial in patients with anterior STEMI. Larger randomized clinical trials examining this treatment strategy are necessary to better define the efficacy and safety of IC eptifibatide.

The editors would like to thank the many members of the cardioAlex 2011 Interventional Cardiology Conference presenting faculty who generously gave their time to ensure the accuracy and quality of the articles in this publication.
Produced proudly in collaboration with ICOM.
- © 2011 MD Conference Express
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.