

Summary
In a session entitled “Emergent Situations in Patients on New Oral Anticoagulants,” a panel of experts discussed the use of novel oral anticoagulants (NOACs) in various clinical situations.
- Thrombotic Disorders
- Arrhythmias
- Interventional Techniques & Devices
- Thrombotic Disorders
- Arrhythmias
- Cardiology
- Interventional Techniques & Devices
In a session entitled “Emergent Situations in Patients on New Oral Anticoagulants,” a panel of experts discussed the use of novel oral anticoagulants (NOACs) in various clinical situations.
PATIENTS WITH RECENT PULMONARY EMBOLISM NEEDING URGENT SURGERY
Marco Cattaneo, MD, Università degli Studi di Milano, Milan, Italy, opened the session with a talk on how he would treat patients with recent pulmonary embolism undergoing urgent surgery. Emphasizing that there are no evidence-based guidelines on how to manage patients on NOACs in this situation, he first laid out the clinical challenge for managing antithrombotic therapy in patients undergoing invasive procedures, which is to balance the risk of post procedural bleeding with continued anticoagulant treatment against the risk of thromboembolism if anticoagulant treatment is suspended.
In patients with pulmonary embolism who are at a high risk of recurrent venous thromboebolism after surgery, Prof Cattaneo suggested considering placing a removable inferior vena cava filter. In terms of NOAC use in high-risk patients who need urgent surgery, he discussed the challenge of and need for quickly reversing the anticoagulant effect.
Of the therapies that may improve hemostasis in patients on NOACs, including prothrombin complex concentrates (PCCs; 3F or 4F), activated prothrombin complex concentrates (aPCCs), recombinant activated factor VII (rFVIIa), hemodialysis (only for dabigatran), and activated charcoal, he said that PCC, aPCC, and rFVIIa are all associated with an increased risk of thrombosis and no evidence that they decrease bleeding. Therefore, he recommended against the use of these hemostatic measures (ie, PCC, aPCC, and rFVIIa) in patients taking NOACs who are at high thrombotic risk and need urgent surgery.
Because of the relatively short half-life of NOACs, one possibility of reducing the bleeding risk in patients needing urgent surgery is to stop administration of NOACs ≥ 24 hours prior to surgery (Table 1) [Healey JS et al. Circulation. 2012].
Risk of Major Bleeding by Timing of Preoperative Medication Discontinuation
Overall, for patients taking NOACs who are at high risk of thromboembolism and need urgent surgery, Prof Cattaneo recommended waiting to perform surgery at least 12 to 24 hours from the last administration of NOACs if the patient has normal renal function. He recommended restarting full-dose NOAC administration as soon as the clinical condition permits.
EVALUATING LABORATORY COAGULATION TEST RESULTS
Peter Verhamme, MD, Department of Cardiovascular Medicine, University of Leuven, Leuven, Belgium, talked about how to use laboratory tests in patients taking the new anticoagulants. Although most people do not require monitoring, he focused on cases in which determining coagulation status may be useful, such as patients presenting to the emergency room with bleeding, acute thromboembolism, and the need for urgent interventions.
For measuring the anticoagulant effect of NOACs, Dr Verhamme walked participants through interpreting coagulation assays for the different types of NOACs and highlighted the different sensitivities of the assays and their ability to measure the anticoagulant effect of different types of NOACs (Table 2) [Heidbuchel et al. Europace. 2013].
Measuring the Anticoagulant Effect of Novel Oral Anticoagulants
As highlighted in Table 2, a sensitive assay may provide information on prothrombin time (PT), activated partial thromboplastin time (aPTT), dilute thrombin time, and Ecarin clotting time. Dr Verhamme emphasized that the international normalized ratio is not validated for providing any information about NOACs and should not be used.
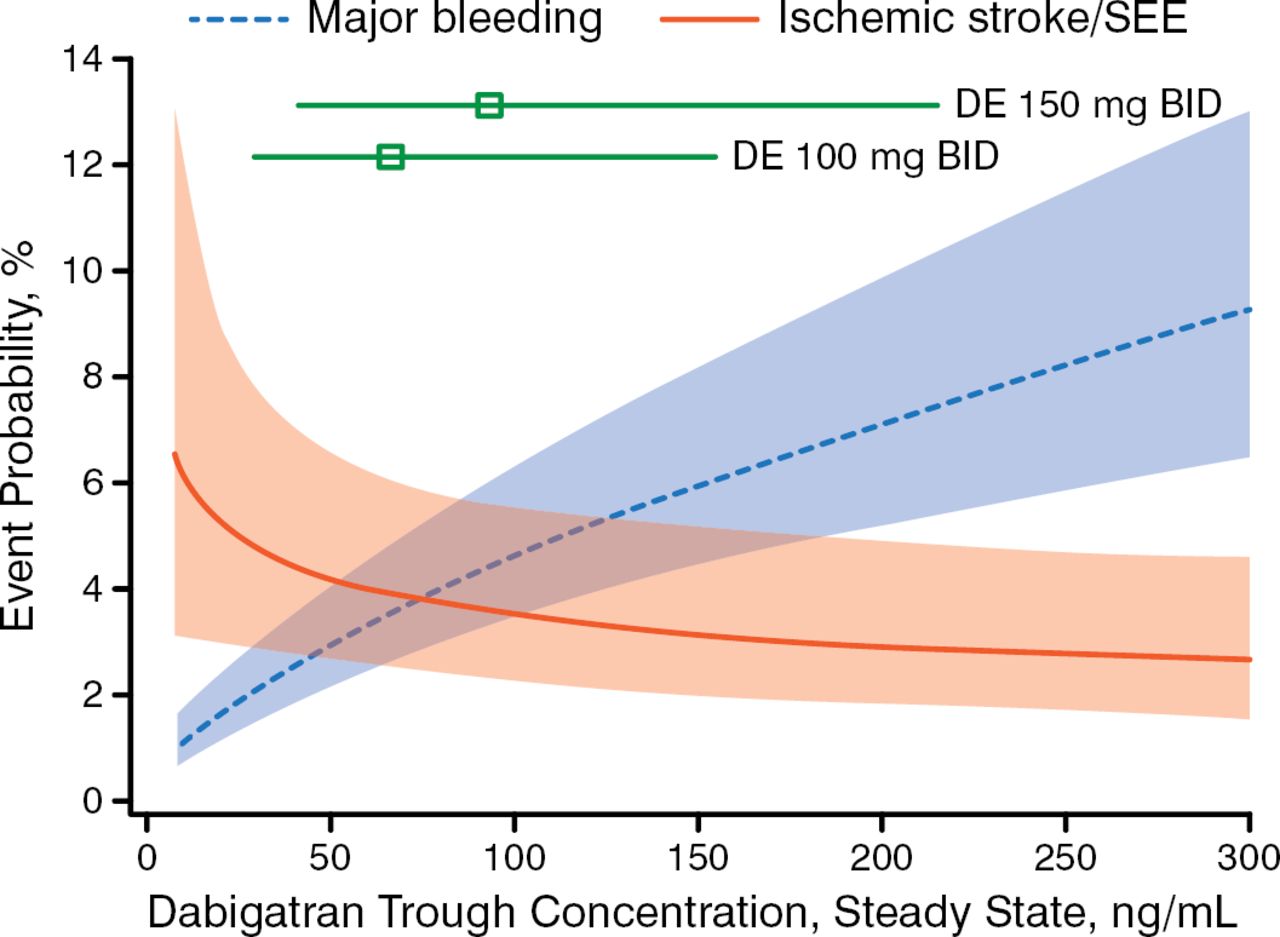
Along with patients who present to the emergency room, other patients for whom measuring the anticoagulant effect of NOACs may be useful are frail patients with multiple comorbidities who are taking multiple medications and remain very concerned with preventing stroke. For these patients, Dr Verhamme showed data on the importance of achieving sufficient trough concentrations of NOACs to reduce stroke risk (Figure 1) [Ruff CT et al. European Society of Cardiology (ESC). 2014; Reilly PA. J Am Coll Cardiol. 2014].

Dabigatran: Trough Level Associated With Bleeding and Stroke
DE, dabigatran; SEE, systemic embolic event.
Adapted from Journal of the American College of Cardiology, 63, Reilly PA et al. The effect of dabigatran plasma concentrations and patient characteristics on the frequency of ischemic stroke and major bleeding in atrial fibrillation patients: the RE-LY Trial (Randomized Evaluation of Long-Term Anticoagulation Therapy). 321–328, Copyright (2014), with permission from American College of Cardiology Foundation.
When measuring the anticoagulant effect of NOACs, he emphasized the importance of knowing when the NOAC was administered relative to the time of taking a blood sample or to the time at which a patient presents to the emergency room. He also emphasized the need for every laboratory and anticoagulation expert to be aware of the relative sensitivity of the PT and APTT assays to rivaroxaban and dabigatran.
MANAGEMENT OF ACUTE BLEEDING COMPLICATIONS
Andrea Rubboli, MD, Ospedale Maggiore, Bologna, Italy, emphasized that bleeding events can be expected with NOACs and talked about the challenge of managing these events given the limited experience to date with these drugs as well as the lack of antidote if bleeding occurs.
Emphasizing that only early and limited data are currently available on reversal agents for NOACs, he reiterated the point made by Prof Cattaneo that the relatively short half-life of NOACs should be considered when managing a planned surgery or bleeding issue.
Of critical importance when using time as an antidote is knowing how rapidly the effect of the NOAC needs to be reversed given the severity and site of bleeding. Answering this question requires knowing the characteristics of the patient, the anticoagulant status (ie, type of anticoagulant, when the last dose was administered, and other drugs taken), the creatinine level, and getting the appropriate anticoagulant laboratory test [Levy S. J Interv Card Electrophysiol. 2014].
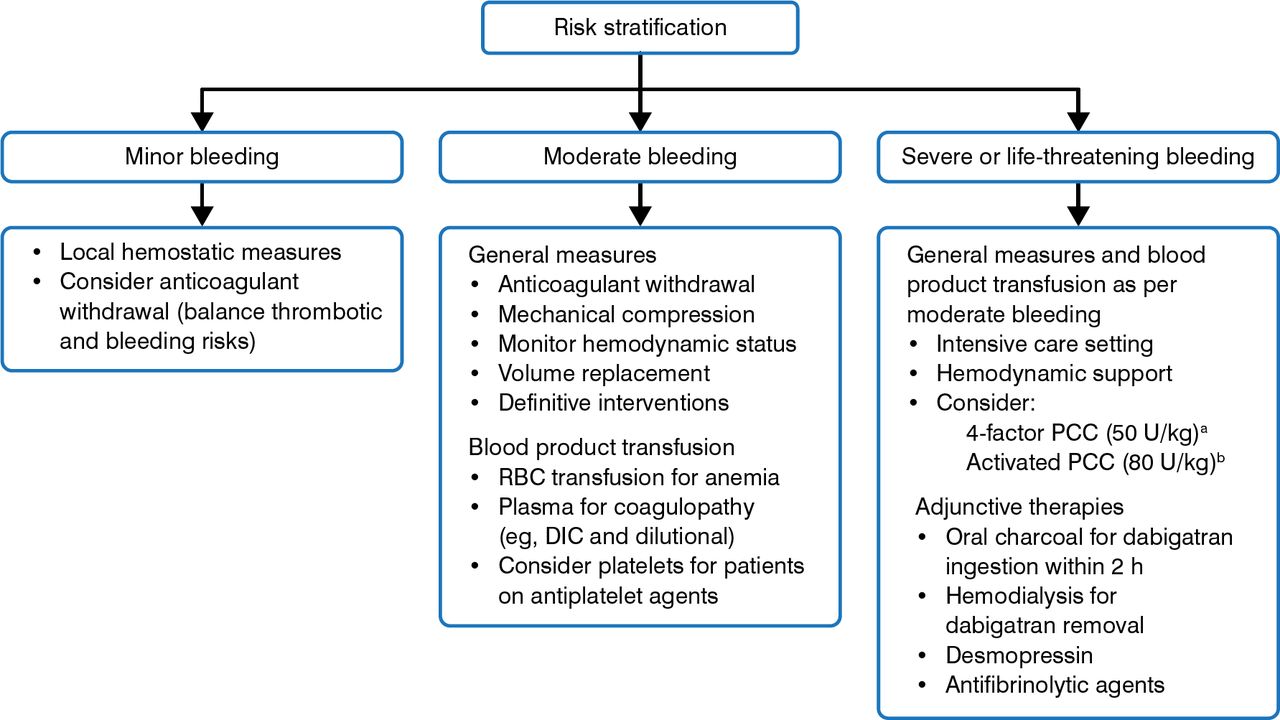
Based on the information, Dr Rubboli emphasized that the management of acute bleeding in patients taking NOACs should be guided by the clinical urgency to reverse anticoagulations and provided an algorithm to help stratify patients according to risk (Figure 2) [Siegal DM et al. Blood. 2014].

Risk Stratification of Patients on Novel Oral Anticoagulants by Severity of Bleeding
DIC, disseminated intravascular coagulation; PCC, prothrombin complex concentrate; RBC, red blood cell.
aPreferred agent for rivaroxaban/apixaban.
bPreferred agent for dabigatran.
Adapted from Blood, Siegal DM et al. How I treat target-specific oral anticoagulant-associated bleeding. 2014;123:1152–1158. With permission of American Society of Hematology. Permission conveyed through Copyright Clearance Center, Inc.
PATIENTS WITH AF AND ACSs WHO REQUIRE PCI
Sven Wassmann, MD, Isar Heart Center, Munich, Germany, ended the session by emphasizing the difficulty of managing anticoagulation with NOACs in patients with atrial fibrillation (AF) and acute coronary syndromes (ACSs) who need to undergo percutaneous coronary intervention (PCI), based on the dearth of clinical evidence in this situation.
Dr Wassmann focused on 2 current guidelines that, to date, can offer some guidance on the use of NOACs in this clinical setting: the 2014 ESC/European Society of European Association for Cardio-Thoracic Surgery guidelines [Windecker S et al. Eur Heart J. 2014] and the ESC/European Heart Rhythm Association (EHRA)/European Association of Percutaneous Cardiovascular Interventions (EAPCI)/Acute Cardiovascular Care Association (ACCA) 2014 consensus document [Lip G et al. Eur Heart J. 2014].
Dr Wassmann provided information on recommendations from each of these 2 guidelines on a number of interconnected therapeutic strategies for ACS, including acute management, long-term management, anticoagulation, platelet inhibition, and PCI/revascularization.
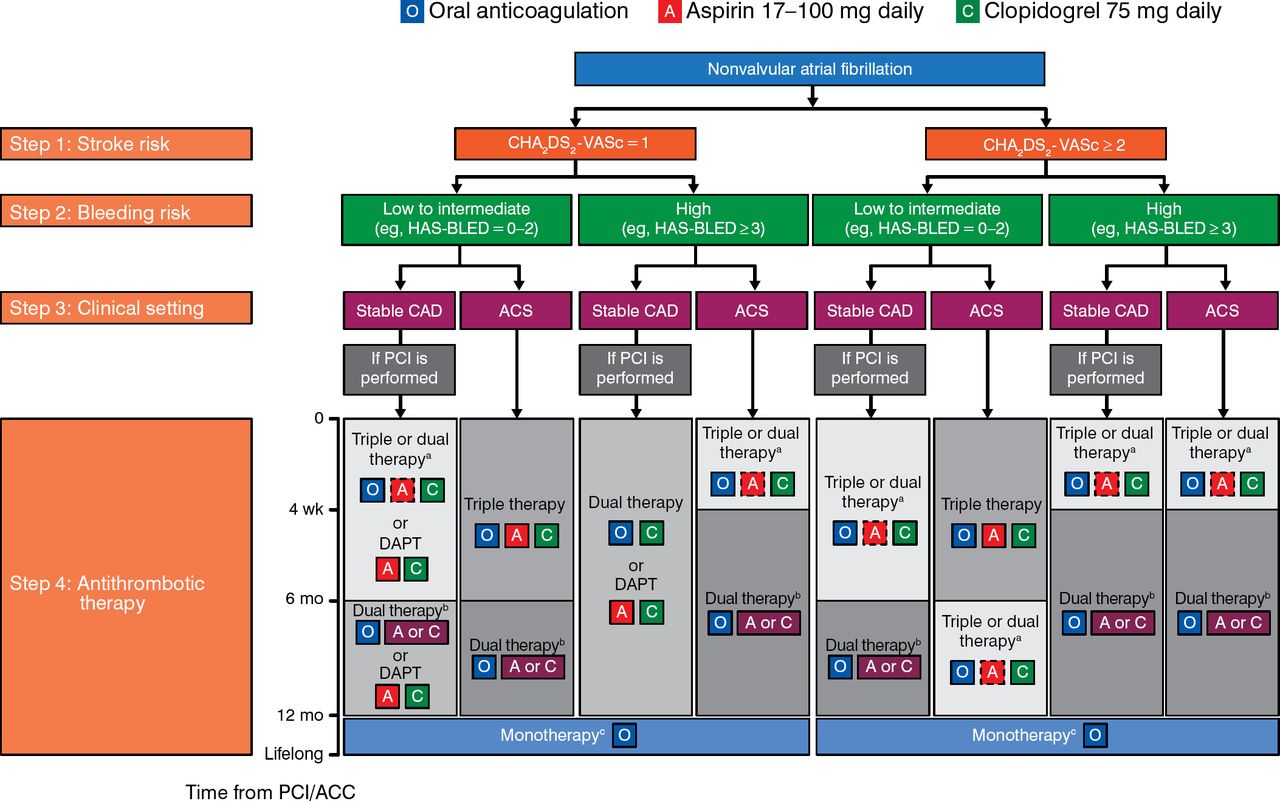
Among the recommendations, he focused on long-term anticoagulant management of patients with AF and ACS by the ESC/EHRA/EAPCI/ACCA 2014 consensus statement, which mandates oral anticoagulation in addition to dual antiplatelet therapy for all patients with a CHA2DS2-VASc score of ≥ 2. Figure 3 illustrates these recommendations in an algorithm.

ESC/EHRA/EAPCI/ACCA 2014 Consensus Statement Algorithm
For step 4, background color and gradients reflect the intensity of antithrombotic therapy (eg, dark background color: high intensity; light background color: low intensity). Solid boxes indicate recommended drugs; dashed boxes indicate optional drugs depending on clinical judgment. A new generation drug-eluting stent is generally preferable over a bare-metal stent, particularly in patients at low bleeding risk (HAS-BLED score 0–2). When vitamin K antagonists are used as part of triple therapy, the international normalized ratio should be targeted at 2.0 to 2.5, and the time in the therapeutic range should be > 70%.
A, aspirin; ACCA, Acute Cardiovascular Care Association; ACS, acute coronary syndrome; C, clopidogrel; CAD, coronary artery disease; DAPT, dual antiplatelet therapy; DES, drug-eluting stent; EAPCI, European Association of Percutaneous Cardiovascular Interventions; EHRA, European Heart Rhythm Association; ESC, European Society of Cardiology; INR, international normalized ratio; O, oral anticoagulation; PCI, percutaneous coronary intervention.
aDual therapy with oral anticoagulation and clopidogrel may be considered in selected patients.
bAspirin as an alternative to clopidogrel may be considered in patients on dual therapy (ie, oral anticoagulation plus single antiplatelet).
cDual therapy with oral anticoagulation and an antiplatelet agent (aspirin or clopidogrel) may be considered in patients at very high risk of coronary events.
Adapted from Lip GY et al. Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: a joint consensus document of the European Society of Cardiology Working Group on Thrombosis, European Heart Rhythm Association (EHRA), European Association of Percutaneous Cardiovascular Interventions (EAPCI) and European Association of Acute Cardiac Care (ACCA) endorsed by the Heart Rhythm Society (HRS) and Asia-Pacific Heart Rhythm Society (APHRS). Eur Heart J. 2014; First published online: 26 August 2014. DOI: http://dx.doi.org.ezp-prod1.hul.harvard.edu/10.1093/eurheartj/ehu298. With permission from European Society of Cardiology.
Dr Wassmann ended his talk and the session by urging centers to set up their own local clinical treatment pathways according to the recommendations based in these guidelines.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.