

Summary
The underlying mechanisms of atrial fibrillation (AF) and its initiation are not well understood, yet catheter ablation can effectively terminate AF in many patients. This article discusses the benefits of ablation for patients with AF.
- Interventional Techniques & Devices Arrhythmias
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Arrhythmias
The underlying mechanisms of atrial fibrillation (AF) and its initiation are not well understood, yet catheter ablation can effectively terminate AF in many patients. Ravi Kishore Amancharla, MD, Health City Cayman Islands, Grand Cayman, discussed the benefits of ablation for patients with AF.
There are 2 major competing theories about the mechanism of AF. The “spatially localized” theory suggests that AF is the result of automaticity or localized reentry, whereas the “spatially meandering” theory suggests that AF is the result of multiple-wave reentry. Dr. Amancharla stated that initiation of AF is likely a result of both focal triggers and abnormal substrate.
Catheter ablation of AF focuses on likely focal triggers, and the method used depends on the location. A majority of foci are located within the pulmonary vein [Haissaguerre M et al. N Engl J Med 1998], as the muscular sleeve of atrial tissue can be found several centimeters into the adjoining region of the vein. By placing multiple catheters into the pulmonary veins, the location of the trigger can be isolated. However, the triggers may not consistently arise from the same location; therefore, the method changes to ablation of the entire segment of the pulmonary vein. Yet, the muscle sleeve can extend deeper into the atrium, so a large portion of the pulmonary vein is disconnected from the atrium, to lower the risk of recurrence due to better isolation of the pulmonary vein. Despite these improvements, the 5-year recurrence rate at a single center was about 30% following a single procedure (Figure 1). According to Dr. Amancharla, these data suggest that ablation works, but multiple procedures are required for sustained success. The inconsistent results of pulmonary vein isolation may be a result of variable anatomy, inaccurate delineation of the ostium and antrum, the inability to produce an enduring transmural lesion without gaps, and targeting the wrong mechanism. Incorporating newer imaging techniques can help limit these issues, as can the use of a cryoballoon, a circular ablation catheter, and contact force ablation catheters.

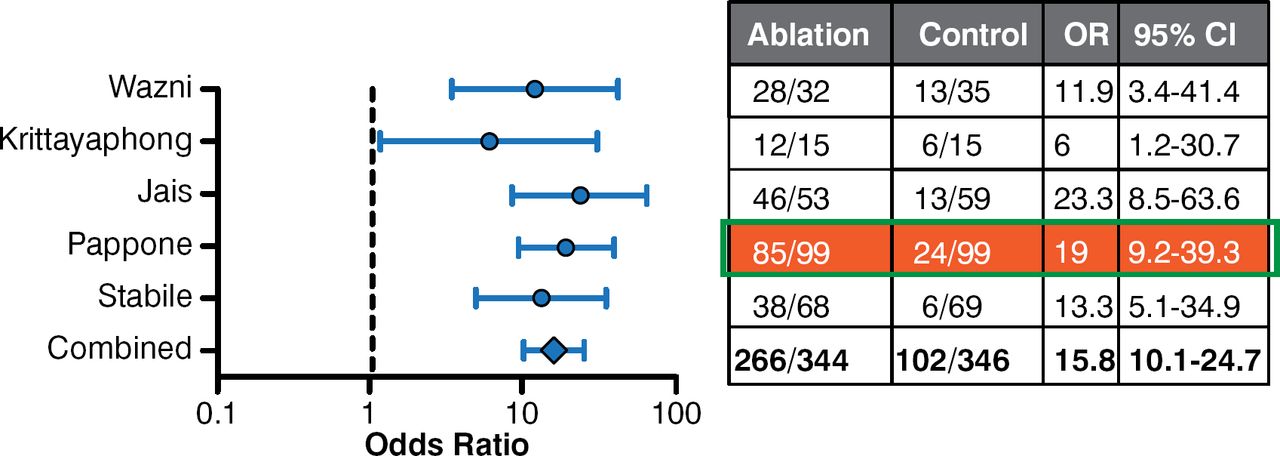
Ablation vs Medical Therapy in Atrial Fibrillation
Reproduced from Piccini JP et al. Pulmonary vein isolation for the maintenance of sinus rhythm in patients with atrial fibrillation: a meta-analysis of randomized, controlled trials. Circ Arrhythm Electrophys. 2009;2:626–633. With permission from Lippincott Williams and Wilkins/Wolters Kluwer Health.
In some patients, other mechanisms beyond the pulmonary vein should be considered, particularly in patients who have persistent to permanent disease. The pulmonary vein plays a lesser role as a trigger for disease in persistent and permanent AF [Fisher JD et al. Pacing and Clin Electrophysiol 2006]. As a result, the ablation strategy should change. The atrial substrate must be identified via electrophysiologic mechanisms and structure.
For linear lesions, areas of the left atrium are identified to reduce the critical mass, which are required for multiple-wave reentry. Commonly used lines include the perimitral and roof lines [Cabrera JA et al. Eur Heart J 2006], which function to compartmentalize the atria into segments that reduce the risk of recurrence.
Targeting complex potentials, as indicated by complex fractionated atrial electrograms (CFEs), is typically used as an adjuvant strategy with pulmonary vein isolation or linear ablation. CFEs are composed of ≥ 2 deflections or a continuous deflection from baseline of a prolonged activation complex over a 10-second recording. However, Dr. Amancharla commented that the opinion of most electrophysiologists is that targeting only CFEs is no longer recommended.
Another method that can terminate persistent AF is alcohol ablation via the Marshall vein, which is a rudimentary structure that connects the proximal coronary sinus to the atrial appendage. However, the Marshall vein also supplies multiple ganglion plexi; therefore, Dr. Amancharla postulated that the mechanism of AF termination is blockade of the autonomic nervous system.
In conclusion, Dr. Amancharla stated that the lesson learned from this stepwise approach of ablation is that up to ∼87% of patients experience AF termination with 3 hours of ablation. Importantly, the trigger is terminated slowly, and the exact trigger may not necessarily be known. However, despite the limitations of ablation, it is still favored over medical therapy in patients who have been failed by an antiarrhythmic agent, according to a systematic review (Figure 1) [Piccini JP et al. Circ Arrhythm 2009].
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.