

Summary
Although mitral valve repair is well established, initial reports of the success of aortic valve repair were mixed. A review of 11 studies from 1990 to 2002, including 761 patients who underwent aortic valve repair, reported that the durability of the repairs was unclear and that patients with rheumatic valvular disease had an increased incidence of recurrence and repair failure [Carr JA, Savage EB. Eur J Cardiothorac Surg 2004]. Since that report, new standardized techniques have been developed for durable aortic valve repair, making it a viable and favorable option when anatomically possible.
- Interventional Techniques & Devices
- Valvular Disease
- Cardiology & Cardiovascular Medicine
- Interventional Techniques & Devices
- Valvular Disease
Although mitral valve repair is well established, initial reports of the success of aortic valve repair were mixed. A review of 11 studies from 1990 to 2002, including 761 patients who underwent aortic valve repair, reported that the durability of the repairs was unclear and that patients with rheumatic valvular disease had an increased incidence of recurrence and repair failure [Carr JA, Savage EB. Eur J Cardiothorac Surg 2004]. However, Edward B. Savage, MD, Cleveland Clinic Florida, Weston, Florida, USA, stated that since that report, new standardized techniques have been developed for durable aortic valve repair, making it a viable and favorable option when anatomically possible.
Conditions that can cause aortic regurgitation (AR) include cusp prolapse, perforation, and retraction. Dilation of the annulus or the sinotubular junction can also lead to regurgitation. The main principle in aortic valve repair is to correct the primary abnormality. The length of the coaptation-free margins should be evened and the height of the leaflets raised, resulting in increased coaptation height.
One repair technique involves shortening the length of the free margin of the leaflet by central plication or by free-margin suspension to match the others [Tamer S et al. Ann Cardiothorac Surg 2013]. In patients with annular dilation, subcommissural annuloplasty can be performed, in which a suture is placed and tightened to pull the bottom together and push the leaflets up. Another way to accomplish this is with commissural plication, in which a suture is placed around the commissure outside the aorta to shrink the annular diameter and push the leaflets together.
A new technique under development in an animal model involves using a ring, which fits beneath the valve with 3 posts fitting into the commissures to match the normal configuration of the aortic root [Rankin JS et al. J Thorac Cardiovasc Surg 2011]. According to Dr. Savage, the ring will reduce the diameter of and stabilize the annulus. One note of caution is that fibrosis might develop on the valve, affecting the leaflets, so long-term follow-up is needed to assess the durability of these devices.
Another repair method, if there is inadequate valve tissue, is augmentation using the patient's pericardium as a patch, which is glutaraldehyde fixed and sutured to the free margin of the leaflet. Good long-term results of this technique have been published, but the patch can calcify and restrict leaflet motion.
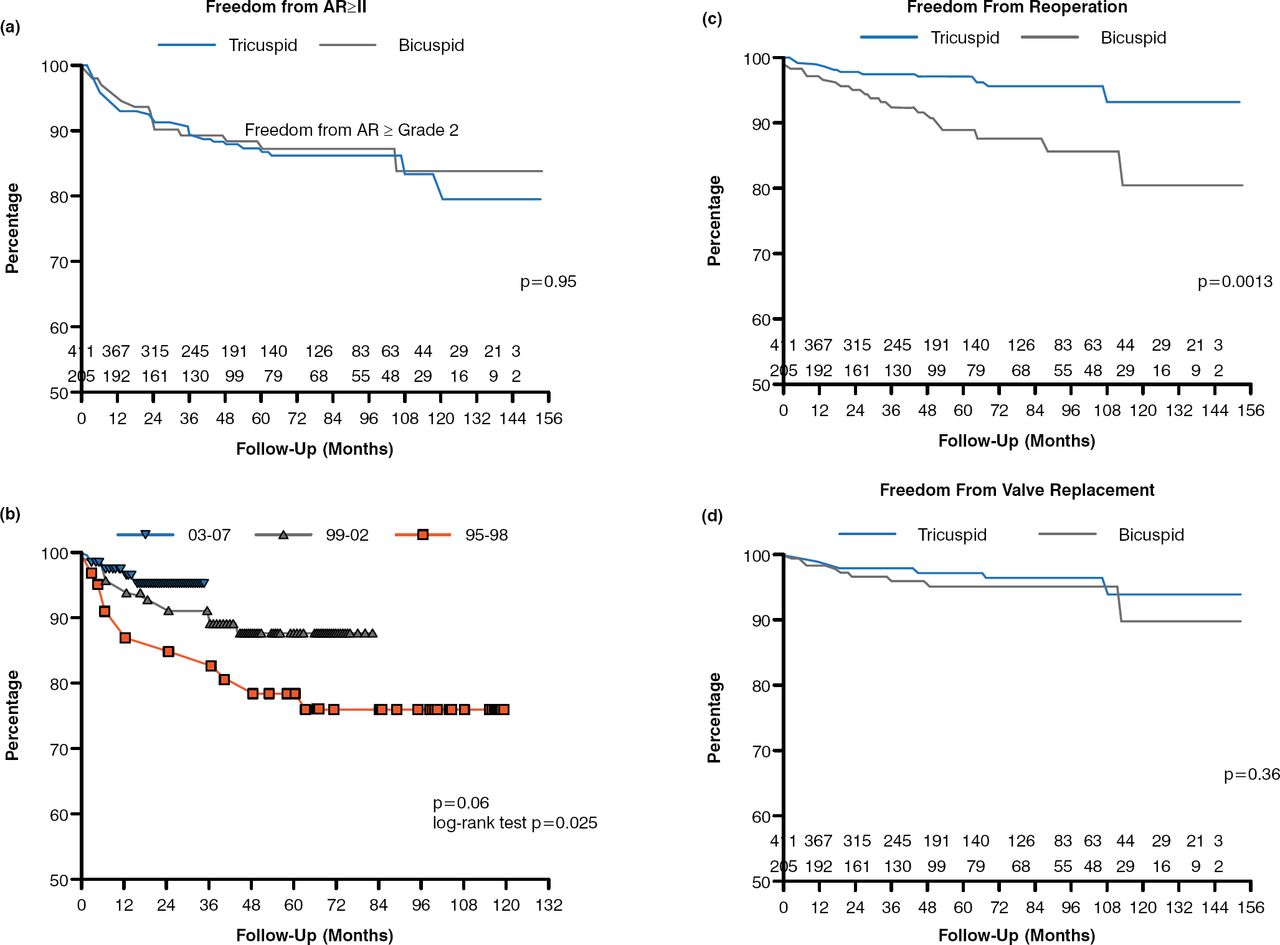
A study evaluating aortic valve repair with cusp or root repair or a combination of both reported comparable freedom from AR greater than or equal to grade 2 in repaired bicuspid and tricuspid valves (p = .95; Figure 1) [Aicher D et al. Eur J Cardiothorac Surg 2010]. There was a significant improvement in freedom from AR greater than or equal to grade 2 for repairs performed during more recent years, demonstrating the influence of valve repair experience (log-rank p = .025). Freedom from reoperation at 10 years was 81% in bicuspid valves and 93% in tricuspid valves (p = .0013), while freedom from valve replacement was 90% in bicuspid valves and 94% in tricuspid valves (p = .36).

Ten-Year Results of Aortic Valve Repair
AR=aortic regurgitation.
Reproduced from Aicher D, Fries R, Rodionycheva S, Schmidt K, Langer F, Schäfers HJ. Aortic valve repair leads to a low incidence of valve-related complications. Eur J Cardiothorac Surg. 2010;37:127–132. With permission from Elsevier.
Dr. Savage concluded that aortic valve repair is durable in appropriate situations and is a viable treatment option. He argued that there may be situations in which aortic valve repair is preferable to mechanical or bio-prosthetic valve replacement.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.