

Summary
This article discusses methods to control and reduce the level of mortality in patients with atrial fibrillation (AF). Dedicated clinics with nurse-led programs addressing of nonstroke-related mortality, ablation, and rate and rhythm control are potential strategies to explore to reduce AF-related cardiovascular outcomes.
- Cerebrovascular Disease
- Heart Failure
- Arrhythmias
- Cardiology
- Cerebrovascular Disease
- Heart Failure
- Arrhythmias
A panel of experts discussed possible methods to control and reduce the level of mortality in patients with atrial fibrillation (AF). Dedicated clinics with nurse-led programs addressing of nonstroke-related mortality, ablation, and rate and rhythm control are potential strategies to explore to reduce AF-related cardiovascular (CV) outcomes.
THE ROLE OF DEDICATED AF CLINICS TO REDUCE STROKE AND MORTALITY IN AF PATIENTS
John Camm, MD, St George's University of London, London, United Kingdom, addressed the role of specialist AF clinics in reducing stroke and mortality in patients with AF. These clinics may improve adherence to AF treatment guidelines [Gorin L et al. Chest. 2011; Nieuwlaat R et al. Am Heart J. 2007]. Suboptimal control of anticoagulant therapy is associated with increased stroke or systemic embolism, major bleeding episodes, and death [Kakkar AK et al. AHA. 2012].
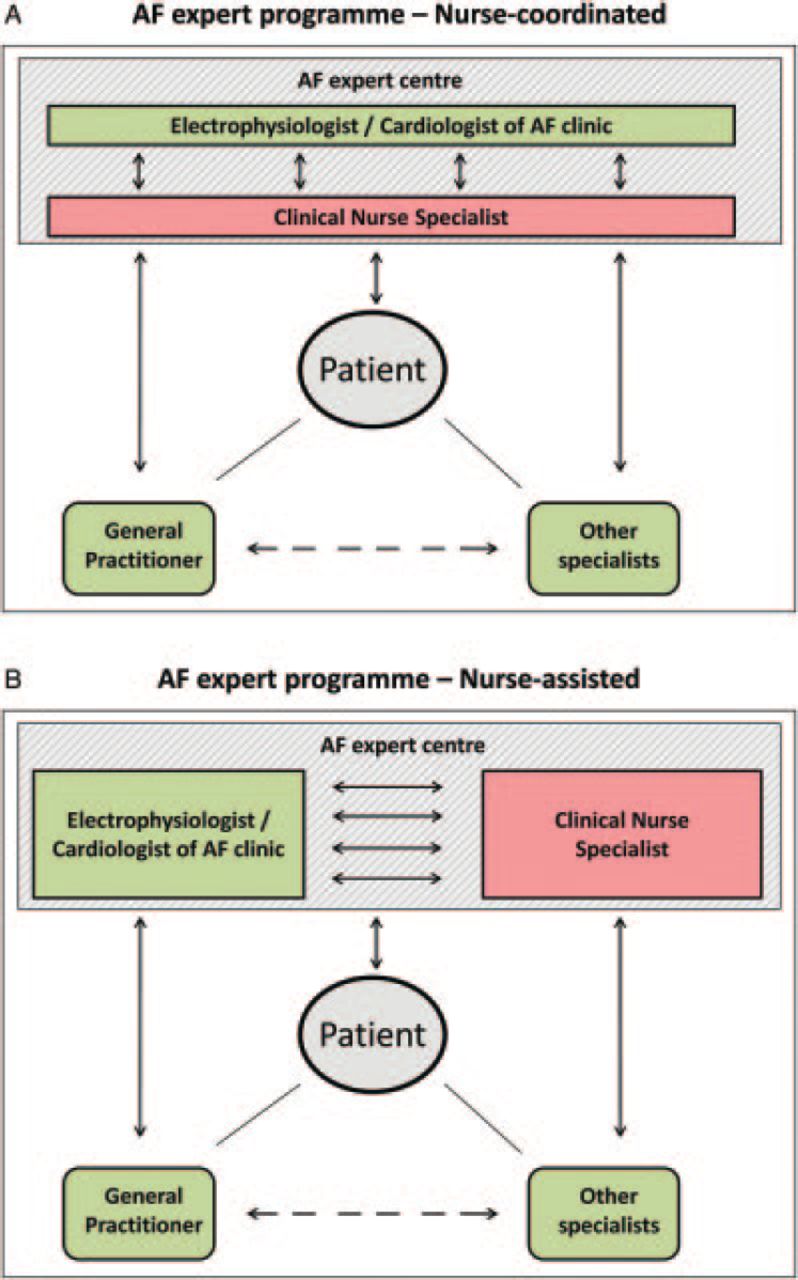
Minimizing undertreatment of AF has been successful via guideline-based care delivered in a nurse-centered interdisciplinary fashion [Berti D et al. Eur Heart J. 2013]. Cardioversion of persistent AF performed by trained nurses yields high rates of patient satisfaction and success at discharge and reduces waiting times for elective procedures [Gillis AM et al. Can J Cardiol. 2008; Boodhoo L et al. Heart. 2004]. The only randomized comparison of usual care versus nurse-coordinated care documented significantly fewer deaths and hospitalizations due to CV causes [Hendriks JM et al. Eur Heart J. 2012]. The advantages as compared with usual care include lower costs and improved survival and quality of life [Hendricks J et al. Europace. 2013].
The design of nurse-centered care is debatable [Berti D et al. Eur Heart J. 2013]. A system where nurses are the main patient-physician conduit (ie, nurse coordinated; Figure 1A) is more popular. Alternatively, nurses can play a central role while being jointly managed by clinicians and clinical nurse specialists (ie, nurse assisted; Figure 1B).

Interdisciplinary AF Expert Programs
AF, atrial fibrillation.
Reproduced from Berti D et al. A proposal for interdisciplinary, nurse-coordinated atrial fibrillation expert programmes as a way to structure daily practice. Eur Heart J. 2013;34:2725–30. With permission from Oxford University Press.
The National Institute for Health and Care Excellence's 2014 guidelines on AF recommended, with some caveats, personalized patient care and information for AF patients [National Clinical Guideline Centre. Atrial Fibrillation: The Management of Atrial Fibrillation. 2014]. This approach will be assessed in the upcoming RACE 4 study [NCT01740037] of > 1700 patients with newly diagnosed AF. The primary end point will be a composite of unplanned hospitalization for any CV cause and CV death.
CV MORBIDITY AND MORTALITY IN AF PATIENTS BEYOND STROKE PREVENTION
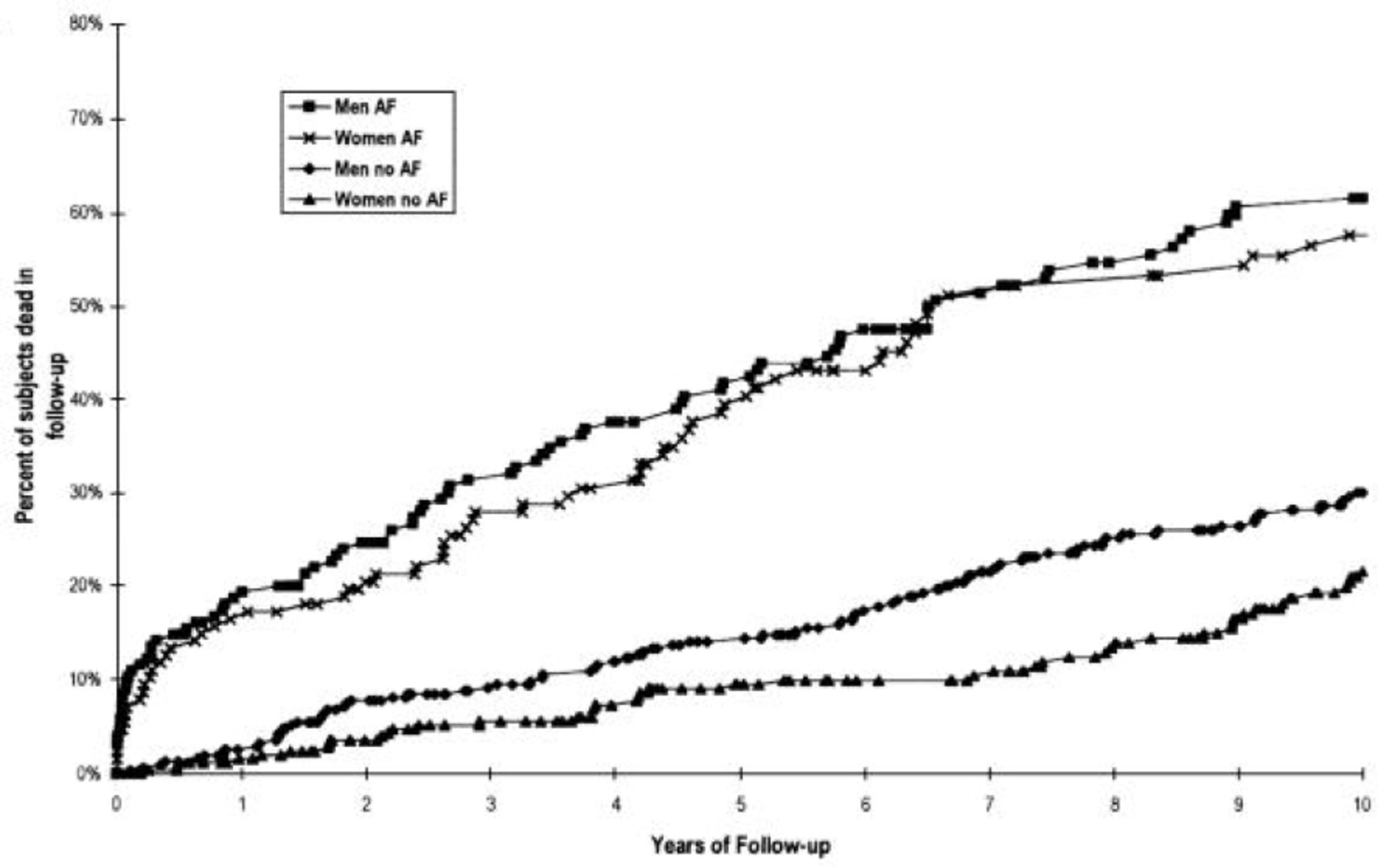
Eloi Marijon, MD, PhD, Paris Descartes University, Paris, France, addressed the association between AF and nonstroke CV outcomes. AF affects an estimated 35 million people globally, with an incidence of 5 million new cases annually [Chugh SS et al. Circulation. 2013]. The Framingham Heart Study revealed that men with AF are twice as likely to die as men without AF, while women with AF are 3 times as likely as those without AF (Figure 2). The authors found that although approximately one-half of the increased risk was due to comorbid CV conditions, AF still independently predicted all-cause mortality after control for confounders and predictors.

Higher Mortality With Atrial Fibrillation: Framingham Study Data
AF, atrial fibrillation.
Reproduced from Benjamin EJ et al. Impact of Atrial Fibrillation on the Risk of Death: The Framingham Heart Study. Circulation. 1998;98:946–52. With permission from Lippincott Williams & Wilkins.
The causal relationship between AF and stroke has led to the development and expanded use of new oral anticoagulants and left atrial appendage occlusion. While reduction in stroke risk continues to be a pressing problem, identification and better understanding of whether there are causal relationships between AF and nonstroke causes of mortality have been explored in large randomized controlled trial populations [Marijon E et al. Circulation. 2013; Roy D et al. N Engl J Med. 2008; Steinberg JS et al. Circulation. 2004]. These studies have demonstrated that in patients receiving anticoagulation treatment, CV mortality still remains the leading cause of death, often due to congestive heart failure (CHF), myocardial infarction (MI), and sudden cardiac death (SCD), not stroke. In one study, stroke constituted only about one-quarter of CV mortality up to 5 years after a first AF event [Piccini JP et al. Eur Heart J. 2014].
The relationship between AF and MI, SCD, and CHF is more complex than it is with stroke. The nearly 2-fold increased risk of MI in patients with AF [Soliman EZ et al. JAMA Intern Med. 2014] is reduced with anticoagulation, suggesting that at least for some patients, coronary embolism may be the cause [Dukes JW et al. JAMA Intern Med. 2014]. Other hypotheses include AF-induced inflammation leading to plaque rupture or simply no causal relationship (ie, only presence of concomitant MI-related risk factors). Whether AF leads to SCD is not definitively known, but studies suggest not [Chen LY et al. JAMA Intern Med. 2013]. CHF is one of the strongest predictors of SCD, and when adjusted for, there appears to be no remaining association between AF and SCD [Marijon E et al. Circulation. 2013; Reinier K et al. JACC Heart Fail. 2014]. AF can be a direct cause of CHF (eg, tachycardia-induced cardiomyopathy). Whether there are other unknown mechanisms by which AF causes CHF is likely but poorly defined.
Dr Marijon concluded by stressing that since AF is directly associated with nonstroke causes of mortality, practitioners should consider estimating the risk of adverse CV outcomes beyond stroke; for example, the CHADS2 score has just been reported to predict broader CV outcomes [Ruwald AC et al. Int J Cardiol. 2014].
AF AND HEART FAILURE: A QUESTION OF MANAGEMENT?
Isabelle Van Gelder, MD, PhD, University Medical Center, Groningen, Netherlands, discussed the management of AF in the setting of concomitant heart failure (HF).
AF may be caused by a primary electrical anomaly that, especially in younger patients, responds well to ablation treatment. Much more common, AF results from long-term atrial remodeling, including enlargement and fibrosis, due to conditions such as hypertension, HF, aging, and diabetes [Wyse DG et al. J Am Coll Cardiol. 2014].
The discovery of an increasing number of risk factors suggests that true “lone” AF is probably extremely rare. Almost all patients presenting with AF have at least one of the reported risk factors for AF (eg, subclinical diastolic HF) [Wyse DG et al. J Am Coll Cardiol. 2014]. These risk factors should be sought and aggressively treated during follow-up. One particular risk factor, HF, has been found to be much more prevalent in AF than previously recognized [Maisel WH, Stevenson LW. Am J Cardiol. 2003]. As demonstrated in the CHARM study, AF carries a much worsened prognosis for HF patients, regardless of whether ejection fraction (EF) is preserved or reduced [Olsson LG et al. J Am Coll Cardiol. 2006].
AF therapy seeks to prevent and reduce symptomatic burden and associated clinical outcomes. Therapy for self-terminating AF is symptom driven and seeks to prevent recurrent episodes. In these patients, catheter ablation is significantly more effective than use of antiarrhythmic medication (log-rank P < .001) [Wilber DJ et al. JAMA. 2010]. Catheter ablation, with repeated procedures as needed for persistent AF, can produce long-lasting protection (≤ 8 years), but it still does not provide a cure [Sorgente A et al. Am J Cardiol. 2012]. In the past, trials have demonstrated that rhythm versus rate control did not affect clinical outcomes. Importantly, rhythm control in these trials did not include catheter ablation; thus, it is unclear whether more effective, modern rhythm control strategies might demonstrate a benefit with maintenance of sinus rhythm.
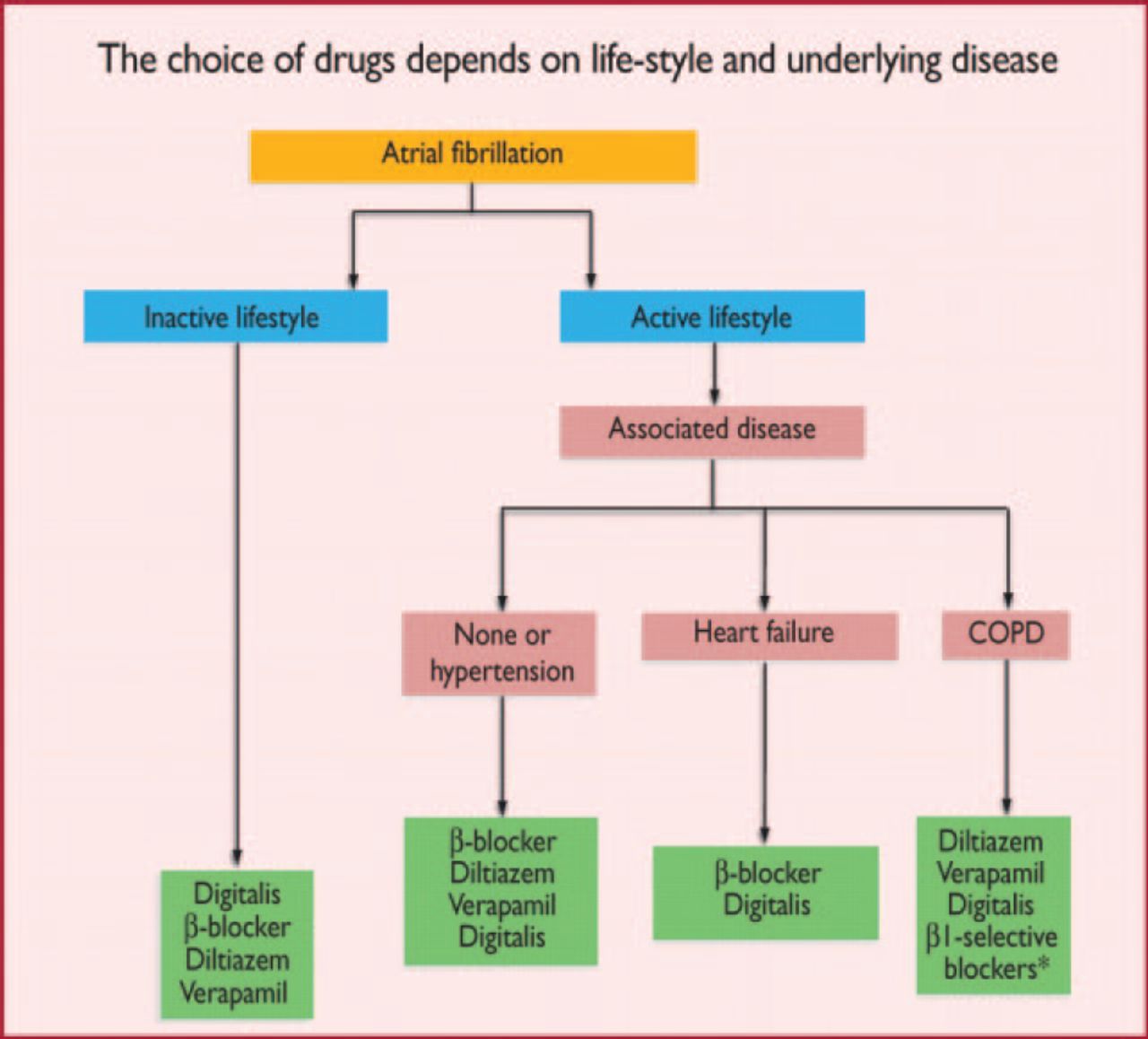
Heart rate control is important when symptoms are present. The choice of medication is lifestyle dependent (Figure 3) [Camm AJ et al. Eur Heart J. 2010].

Choice of Heart Rate Control Medication
COPD, chronic obstructive pulmonary disease.
Reproduced from Camm AJ et al. Guidelines for the management of atrial fibrillation. The Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC). Eur Heart J. 2010;31:2369–429. With permission from Oxford University Press.
Note that the benefits of β-blockers in HF were studied in patients in sinus rhythm, not AF. Reductions in CV outcomes have been reported for bisoprolol and nebivolol in those with sinus rhythm, with no difference found in those with AF [Mulder BA et al. Eur J Heart Fail. 2012; Lechat P. Circulation. 2001]. The European Society of Cardiology 2012 guidelines—which recommended the use of both β-blockers and angiotensin-converting enzyme inhibitors for patients with EF ≤ 40% [McMurray JJV et al. Eur Heart J. 2012]—were based on these studies enrolling patients in sinus rhythm.
Digoxin has been associated with increased AF-related mortality [Corley SD et al. Circulation. 2004], CV mortality, and all-cause mortality [Turakhia MP et al. J Am Coll Cardiol. 2014; Whitbeck MG et al. Eur Heart J. 2013]. Reexamination of this association has yielded conflicting results. Until this hypothesis can be properly tested, these observational data should not discourage use of digoxin in all AF patients. Digoxin remains useful in the treatment of conditions like AF, with low blood pressure, difficult rate control, and frequent HF hospitalizations.
Recent trials of lifestyle management among obese subjects with AF have demonstrated not only reduced weight circumference and body mass index but also decreased scores of symptom burden and severity [Abed HS et al. JAMA. 2013]. This reinforces the view that early and comprehensive lifestyle interventions are needed to reduce the prevalence of AF.
IMPROVING OUTCOMES THROUGH EARLY RHYTHM CONTROL THERAPY
The importance of early intervention with modern therapies was expanded on by Paulus Kirchhof, MD, University of Birmingham, Birmingham, United Kingdom. Dr Kirchhof highlighted that the increased risk of AF-related death is especially evident early following the first episode of AF, even when patients receive optimal anticoagulation and heart rate control therapy.
What makes this period so dangerous is not known. AF is a complex phenomenon that influences the cardiac calcium load, which affects the structural and hemodynamic loops. These effects can exacerbate AF, which can lead to chronic atrial dilation. The interplay between AF and atrial dilation can produce recurrent A F. Chronic dilation can induce fibrosis, which also exacerbates AF. Most important, these long-standing alterations can occur within weeks, if not hours. This raises the hypothesis whether early rhythm control might reduce AF-related complications. As mentioned, while prior studies have not supported a benefit of rhythm control compared to rate control, Dr Kirchhof highlighted that subjects enrolled in many of these studies probably had longer-standing AF and that rhythm control during the period of these trials was less effective [Hohnloser SH et al. N Engl J Med. 2009; Roy D et al. N Engl J Med. 2008; AFFIRM Investigators. J Am Coll Cardiol. 2003; Carlsson J et al. J Am Coll Cardiol. 2003; AFFIRM Investigators. N Engl J Med. 2002; Van Gelder IC et al. N Engl J Med. 2002; Hohnloser SH et al. Lancet. 2000], but none of them was targeted at the early disease stages. This may have been one of the reasons why the outcome of the prior trials was neutral.
In support of these data, the prospective, randomized, open, blinded outcome EAST trial [Kirchhof P et al. Am Heart J. 2013] is being conducted by Prof Kirchhof and colleagues to test the hypothesis that a safely delivered, more effective antiarrhythmic regimen (including catheter ablation and antiarrhythmics) can prevent major complications of death, stroke, and HF as compared with usual care. More than 50% of the required patients have been enrolled (www.easttrial.org).
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.