

Summary
This article presents the case of a 56-year-old Bahamian woman successfully treated by coil embolization for anomalous right coronary artery (RCA) arising from the pulmonary artery.
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Cardiology & Cardiovascular Medicine
- Cardiology Clinical Trials
- Interventional Techniques & Devices
Bimal Francis, MD, DM, Bahamas Interventional Cardiology Center, Nassau, Bahamas, presented the case of a 56-year-old Bahamian woman successfully treated by coil embolization for anomalous right coronary artery (RCA) arising from the pulmonary artery. The woman arrived at the cardiology center with very limiting palpitations, dizziness, dyspnea, and chest pain with minimal exertion. Her medical history revealed that she had had asthma with chest pain, palpitations, and diaphoresis since childhood, hypertension for 10 years, and diabetes for 1 year. A physical examination found normal vital signs, a body mass index of 33 kg/m2, and mild respiratory distress at rest, accompanied by fine crackles at the base of both the left and right lungs. Laboratory results were also normal. Multiple unifocal premature ventricular beats were noted on electrocardiography (ECG). The baseline ECG of the sinus beats showed a right bundle branch block pattern. Echocardiography showed left ventricular function of ∼ 50%. There was no significant mitral regurgitation, no wall movement anomaly, and no abnormal flows.
Because the patient could not be stabilized, coronary angiography was scheduled. The results showed a dilated left coronary artery retrogradely filling a tortuous and dilated RCA through giant collateral vessels. The patient had no other physical cardiovascular signs; there were no murmurs. The RCA was grossly dilated, but the flow was reasonably good. The RCA was draining anomalously into the pulmonary artery, creating a steal effect. The patient tolerated the angiographic study fairly well; however, on returning to the ward, her symptoms worsened, and she was referred to a cardiothoracic surgery team, who determined that she was a poor candidate for surgery and anesthesia.
It was decided to palliate her symptoms by percutaneous closure of the RCA with coil embolization. Eventually 3 coils were put in place. The procedure was well tolerated, with no cardiac enzyme elevation. A 2-dimensional Doppler echocardiographic image revealed posterior ventricular hypokinesia, but the Doppler image detected no abnormal color flowing across the pulmonary artery; the ejection fraction of the patient was 48%. The patient was prescribed antiarrhythmic and antiplatelet medications, β-blockers and angiotensin receptor blockers, and angina medication for cardiac symptoms. She also received treatment for her diabetes and asthma.
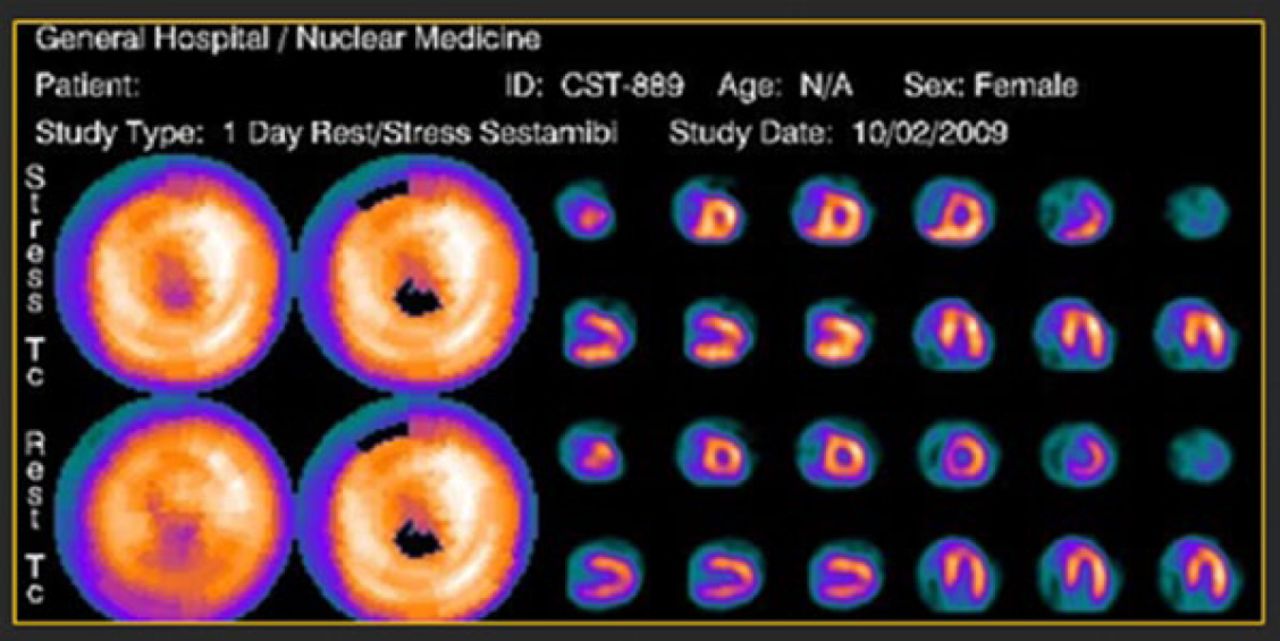
In the first week following embolization, chest pain and shortness of breath lessened in frequency and severity. Physiotherapy improved her ability to walk by Week 3. A dipyridamole technetium sestamibi (Cardiolite; Lantheus Medical Imaging, North Billerica, Massachusetts) stress test showed no inducible ischemia, normal wall motion, and an ejection fraction of 68% (Figure 1).

Dipyridamole Technetium Sestamibi (Cardiolite) Stress Test
Reproduced with permission from B. Francis, MD.
Three months after the procedure, the patient was readmitted for respiratory failure from severe asthma. Two years after the procedure (October 2011), she reported chest pains, which were relieved with glyceryl trinitrate. Right and left catheterization was repeated at this time. Angiography showed no atherosclerotic disease, no migration of coils, no recanalization or leak into the pulmonary artery, and an essentially normal ejection fraction of 65%.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.