

Summary
Use of excimer laser atherectomy (ELA) as an adjunct to percutaneous transluminal angioplasty (PTA, also known as balloon angioplasty) is superior to PTA alone in patients with peripheral artery disease who experience artery narrowing following stent implantation (in-stent restinosis [ISR]). This article discusses the results from the Randomized Study of Laser and Balloon Angioplasty Versus Balloon Angioplasty to Treat Peripheral In-Stent Restenosis [EXCITE ISR; NCT01330628].
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Coronary Artery Disease
- Cardiology
- Cardiology Clinical Trials
- Interventional Techniques & Devices
- Coronary Artery Disease
- Cardiology
Use of excimer laser atherectomy (ELA) as an adjunct to percutaneous transluminal angioplasty (PTA, also known as balloon angioplasty) is superior to PTA alone in patients with peripheral artery disease (PAD) who experience artery narrowing following stent implantation (in-stent restinosis [ISR]).
The results from the Randomized Study of Laser and Balloon Angioplasty Versus Balloon Angioplasty to Treat Peripheral In-Stent Restenosis [EXCITE ISR; NCT01330628] randomized trial were described by Eric J. Dippel, MD, Genesis Heart Institute, Davenport, Iowa, USA.
Treatment of PAD using stent implantation to retain arterial diameter is effective but ISR occurs in 30% to 40% of cases in the 2 years following the procedure. ISR is typically treated with PTA; however, the recurrence of ISR is common following PTA.
The prospective, randomized EXCITE ISR trial was undertaken to evaluate the safety and efficacy of ELA used along with PTA vs PTA alone in treating femoropopliteal ISR. Most ELA procedures used a dedicated laser atherectomy catheter (Turbo-Elite). The inclusion and exclusion criteria of the trial were designed to randomize patients frequently encountered during clinical practice (Table 1).
Inclusion and Exclusion Criteria
The trial randomized 250 patients in whom lesions were suitable. Patients were randomized 2:1 to receive ELA + PTA (n = 169) or PTA (n = 81). The primary safety end point of 30-day major adverse events (death, unplanned major amputation, revascularization of the lesion) was assessed in 155 and 73 patients in the ELA + PTA and PTA group, respectively. The primary efficacy end point (6-month freedom from clinically proven target lesion revascularization [TLR]) was assessed in 117 ELA + PTA patients and 56 PTA patients.
Baseline demographics concerning age, sex, clinical parameters, and lesion assessments were similar, with the exception of more extensive calcification in the ELA + PTS group (27% vs 9%; P = .002).
Procedural success was significantly greater for and residual stenosis was significantly less in the ELA + PTA group (94% vs 83%; P = .03 and 5% vs 14%; P = .02). The need for TLR in the year following surgery was significantly less for those receiving ELA + PTA (P < .003). One-year survival and freedom from major adverse events was significantly higher in those receiving ELA + PTA (P < .005 and P < .001, respectively).
ELA + PTA compared with PTA alone was associated with less TLR (5% vs 16%; P = .008), dissection (8% vs 17%; P = .03), > Grade C (2% vs 7%; P = .08), bailout stenting (4% vs 11%; P = .02), thrombosis (1% vs 3%; P = .25), and abrupt closure (0% vs 1%; P = .23). PTA alone was associated with decreased embolization (8% vs 5%; P = .47).
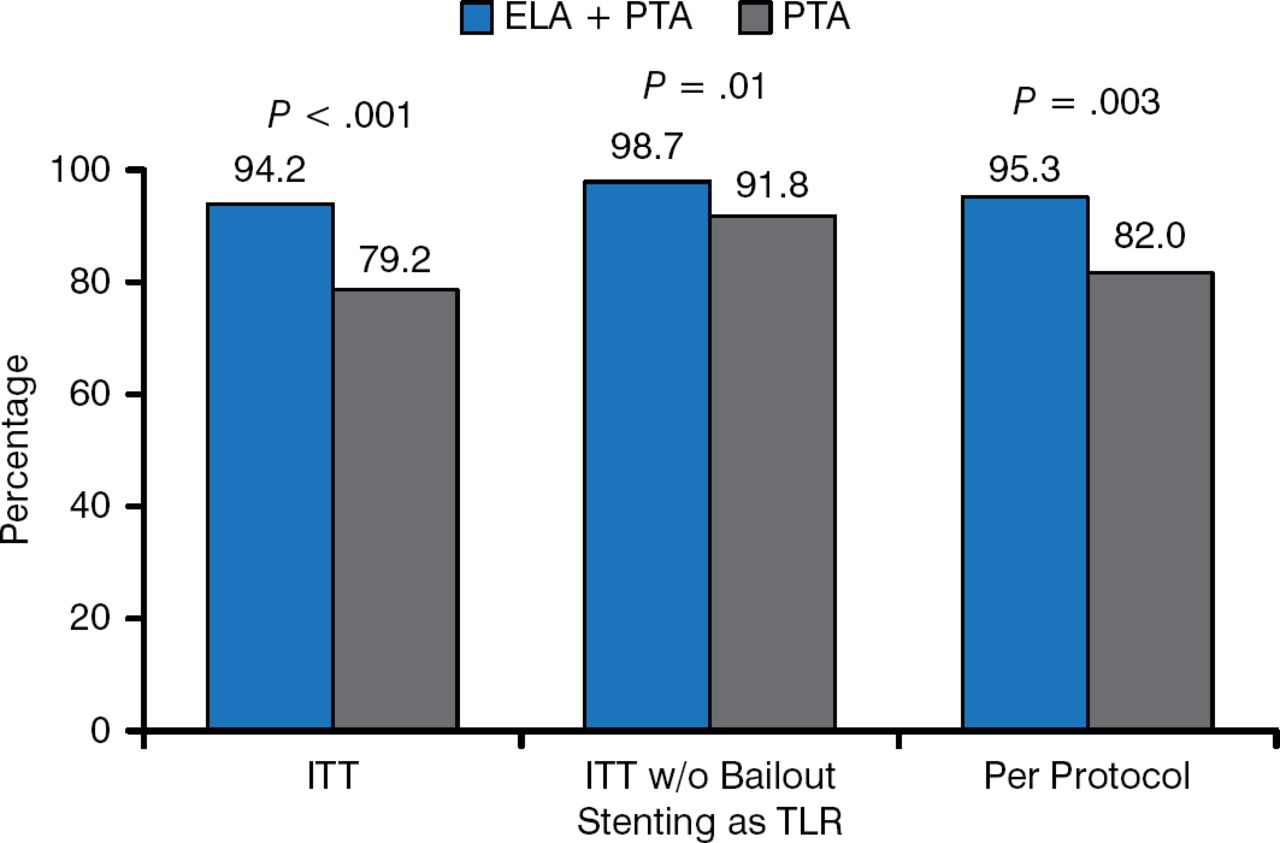
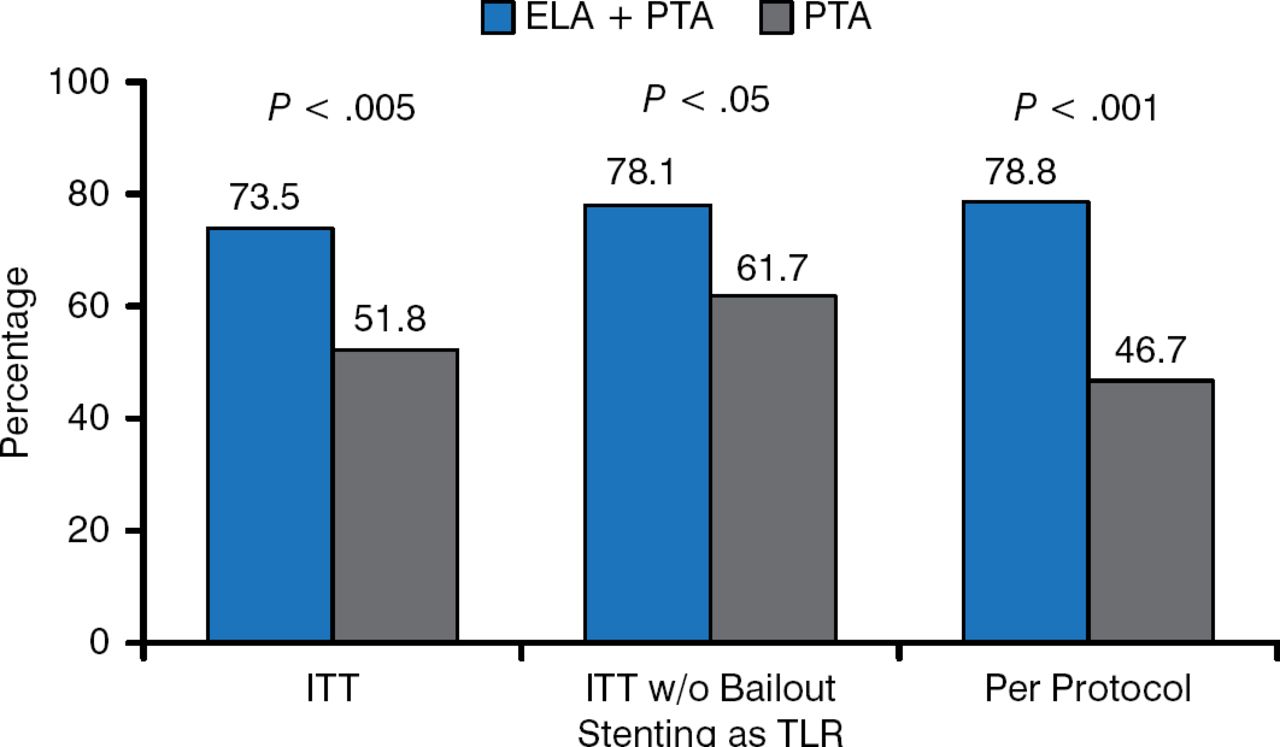
The primary safety and efficacy end points significantly favored ELA + PTA (Figures 1 and 2).

Primary Safety End Point
ELA, excimer laser atherectomy; ITT, intention-to-treat; PTA, percutaneous transluminal angioplasty; TLR, target lesion revascularization.
Reproduced with permission from EJ Dippel, MD.

Primary Efficacy End Point
ELA, excimer laser atherectomy; ITT, intention-to-treat; PTA, percutaneous transluminal angioplasty; TLR, target lesion revascularization.
Reproduced with permission from EJ Dippel, MD.
The advantage of ELA + PTA over PTA held following a battery of subgroups included those based on age, diabetes, prior ISR, artery occlusion, artery diameter, lesion length, and other parameters.
Thus, ELA + PTA treatment of ISR was found to be superior to PTA for the treatment of femoropopliteal ISR involving complicated lesions. Large scale trials are needed to determine if this should be considered standard of care in patients with femoropopliteal ISR.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.