

Summary
This article discusses the diagnosis and management of malignant lesions of the eyelids, orbit, and lacrimal system.
- Head & Neck Cancers
- Eye Cancer
- Ophthalmic Surgery
- Head & Neck Cancers
- Eye Cancer
- Ophthalmology
- Ophthalmic Surgery
In this special session, experts discussed the diagnosis and management of malignant lesions of the eyelids, orbit, and lacrimal system.
Bita Esmaeli, MD, Orbital Oncology and Ophthalmic Plastic Surgery Program, Department of Plastic Surgery, MD Anderson Cancer Center, Houston, Texas, USA, began the session with a discussion of sebaceous carcinoma, a rare but deadly neoplasm that can be difficult to diagnose and treat. It accounts for < 5% of eyelid (mostly upper-lid) cancers in the United States, but is higher in other parts of the world, particularly Asia. Recurrent chalazion or persistent unilateral blepharoconjunctivitis that persists after conservative treatment should be biopsied. Sebaceous carcinoma has a propensity for pagetoid intraepithelial neoplasia and can metastasize to other structures if untreated.
Surgery is mainstay local treatment for sebaceous carcinoma of eyelid. Dr Esmaeli recommends sentinel lymph node biopsy or strict regional lymph node surveillance for patients with eyelid sebaceous carcinomas that are T2b or more advanced (tumors with dimension ≥ 10 mm and/or involving the full thickness of the eyelid). Treatment of metastatic disease may include a combination of chemotherapy, radiation, and surgery. High surveillance is needed following surgery because sebaceous carcinoma can not only recur locally in the eye area but also lead to regional lymph node or systemic metastasis, usually during the first 5 years after surgical treatment, but very late metastasis has also been reported.
Jerry A. Shields, MD, Oncology Service, Wills Eye Hospital, Philadelphia, Pennsylvania, USA, discussed management approaches to extraocular extension (EOE) of uveal melanoma.
Many patients with EOE uveal melanoma already have subclinical metastases, usually in the liver, and aggressive treatment to the primary uveal or orbital melanoma seems unwarranted. Depending on clinical findings (the size of the intraocular and orbital component, the tumor location, or the results of orbital magnetic resonance imaging [MRI]), one option might be exenteration of the eye. Management techniques might include plaque radiotherapy, modified enucleation, or eyelid-sparing or sacrificing exenteration. The most common management approach used today is plaque radiotherapy.
Regardless of the presence of EOE, uveal melanoma can be treated with enucleation or modified enucleation by way of a lateral orbitotomy. Orbital exenteration is an appropriate procedure for unresectable malignant tumors, and it can be performed with either lid sparing to achieve more rapid healing or lid sacrificing for massive EOE [Shields JA et al. Ophthal Plast Reconstr Surg. 2001]. Exenteration is not usually necessary and should be reserved for massive EOE or to improve quality of life. Survival prognosis is unaffected, however.
Carol Shields, MD, Oncology Service, Wills Eye Hospital, Philadelphia, Pennsylvania, USA, reviewed myths and facts about conjunctival melanoma. The incidence of conjunctival melanoma is increasing at a rate that appears to coincide with the increasing rate for cutaneous melanoma, suggesting a possible link to a sunlight-related etiology [Yu GP et al. Am J Ophthalmol. 2003]. During the past 27 years, conjunctival melanoma has increased 300% in white men, especially in those > 60 years old. Mortality is high among individuals with tumors > 2 mm, and in those with tumors in the fornix, caruncule (80% death rate at 4 years), and orbit. The risks of metastasis and death are higher in cases of de novo disease [Shields CL et al. Ophthalmology. 2011]. Inadequate surgical intervention has been shown to increase the risks of local recurrence and metastatic death [Damato B and Coupland SE. Eye (Lond). 2009].
Conjunctival melanoma arises from primary acquired melanosis (PAM; 70%), nevus (15%), and de novo (15%). PAM is characterized by a painless, flat brown spot and is typically found on only one eye. The risk for PAM progression to melanoma is greater in larger (> 1 clock hour) lesions than in those with severe vs mild or no atypia. Cautious, long-term follow-up is advised for all patients with PAM. Alcohol-assisted removal of the epithelium, topical mitomycin-c (MMC) followed by cryotherapy, topical interferon alfa-2b, and 5-fluorouracil (SFU0) are all effective treatments.
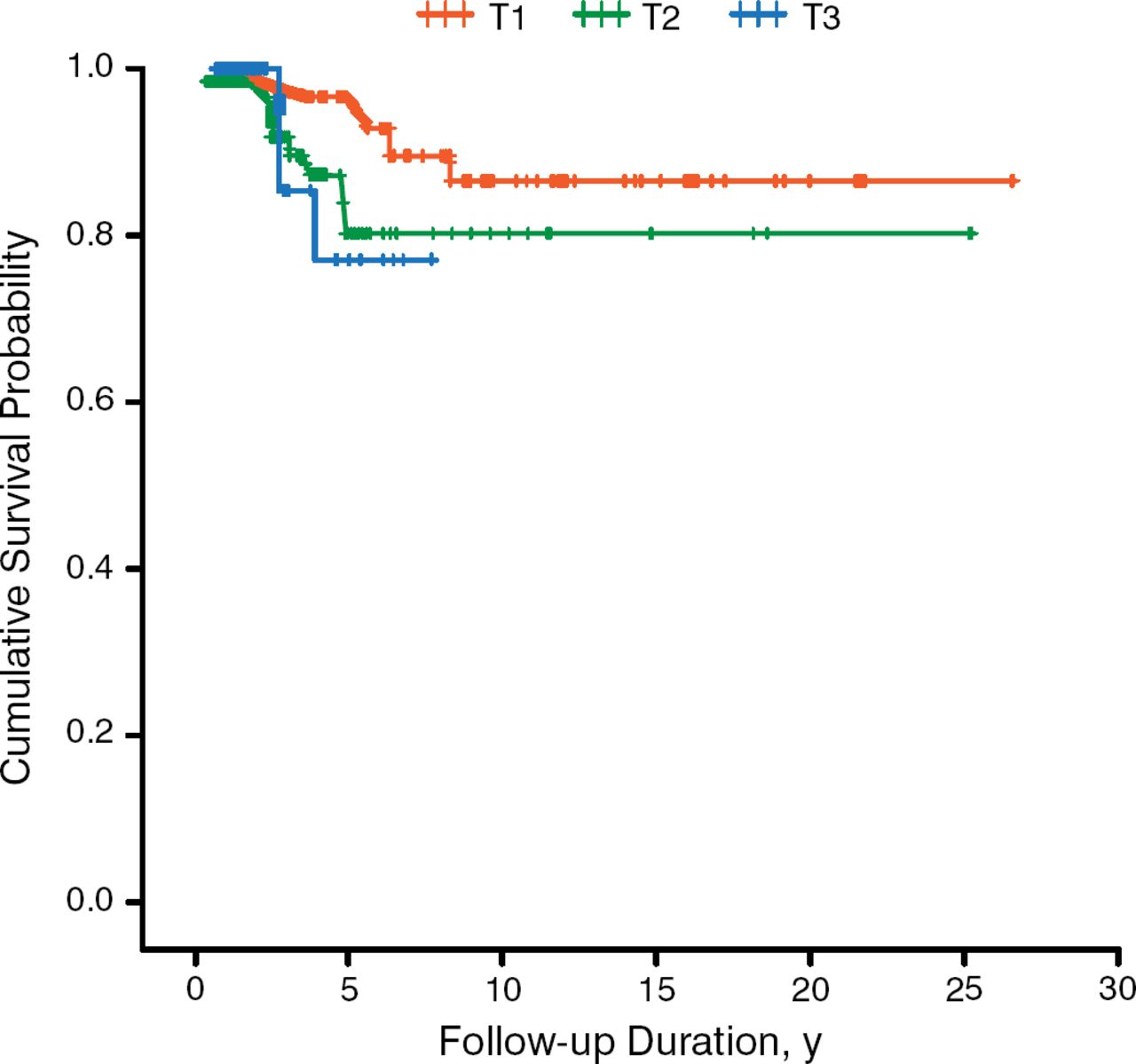
Conjunctival melanoma that is thin and localized to the corneal limbus and bulbar conjunctiva areas of the eye usually has a good prognosis, whereas large, diffuse tumors, located in the fornix, tarsal, or caruncle areas, have poor prognosis. Melanoma classified as T2 and T3 showed higher rates of local recurrence, regional and distant metastasis, and death compared with T1 tumors [Shields Cl et al. Ophthal Plast Reconst Surg. 2012; Figure 1].

Cumulative Survival Probability of T1, T2, and T3 Melanoma
Adapted from Shields CL et al. American Joint Committee on Cancer (AJCC) Clinical Classification Predicts Conjunctival Melanoma Outcomes. Ophthal Plast Reconstr Surg. 2012;28:313–323. With permission from The American Society of Ophthalmic Plastic and Reconstructive Surgery, Inc.
Scott M. Goldstein, MD, Wills Eye Hospital, Philadelphia, Pennsylvania, USA, presented an overview of rhabdomyosarcoma. Rhabdomyosarcoma is a malignant tumor of the muscle arising from mesenchymal skeletal muscle progenitors typically found in the head, neck, and genitourinary tract. Although rare, it is the most common primary pediatric orbital malignancy. Rhabdomyosarcoma can be divided into the following histological subsets: embryonal (50% to 60% of cases), alveolar (20% to 30%), pleomorphic (< 1%), and botryoid (very rare).
Treatment is based on staging: chemotherapy only for stage I, chemotherapy and radiation for stage II, chemotherapy and radiation at higher doses for stage III, and intensive vincristine, dactinomycin, and cyclophospha-mide (VAC) and radiation therapy for stage I V. There is a 17% chance of recurrence within 18 months, but prognosis is favorable for the following conditions: orbital tumor, age 1 to 10 years at diagnosis, female sex, embryonal type, and tumor < 5 cm in diameter.
Molecular targeting is at the forefront of cancer treatment, given that cancer is a “genetic disease.” Alveolar rhabdomyosarcoma often has a PAX3 or PAX7 trans-location with the FKHR (FOX01) gene, which is associated with a worse outcome. A genetic defect has not been assigned to embryonal rhabdomyosarcoma. In the future, molecular testing for tumor type may be helpful in classifying the tumor and determining prognosis. MRI and diffusion-weighted imaging may also be helpful in identifying orbital lesions. Currently, orbital proton beam radiotherapy is being used as a treatment for rhabdomyosarcoma at Wills Eye. Molecular therapy for this disease is still being researched.
David T. Tse, MD, FACS, Bascom Palmer Eye Institute, Miami, Florida, USA, reviewed the optimal therapeutic approach to treating adenoid cystic carcinomas (ACCs) of the lacrimal gland.
ACC, the most common nonlymphoid malignant tumor of the lacrimal gland, accounts for 25% to 30% of epithelial tumors and confers the worse prognosis among this type of tumor. Exenteration with or without bone removal plus radiation comprise the conventional treatment. Survival following initial surgery is < 50% at 5 years and < 20% at 10 years. There is a 55% to 80% recurrence rate.
Poor long-term survival in patients with ACC can be attributed to the complex nature of the orbital anatomy, aggressive biological behavior of the disease, and eventual intracranial involvement, which is the principal cause of death. Advancements in conventional therapy have not improved disease-free survival, and there have been no improvements in controlling occult metastases—even after surgery and radiation have achieved local disease control. Thus, treatment is shifting toward a new approach: neoadjuvant intra-arterial chemotherapy. This treatment is given to patients likely to develop metastatic disease.
The therapy allows for a higher drug dose delivery (cisplatin or adriamycin) that can overwhelm tumor repair mechanisms, induce tumor necrosis, minimize dissemination of viable tumor cells during surgical manipulation, reduce tumor size, and eradicate tumor cells that may have escaped the orbit confines. In one group of patients (n = 8), cumulative 10-year disease-free survival was 100%. Longest survival was 25 years. In a second group (n = 11), cumulative survival was 72%.
Following globe-sparing tumor resection, the patient receives modulated radiation therapy and 4 cycles of cisplatin and adriamycin. The resected tumor undergoes molecular and genomic profiling to guide choice of therapy, assess recurrence risk, and determine genetic markers for further prognostic clues. This protocol has made it possible to characterize the lacrimal gland ACC cell culture, serves as a tool for in vitro and in vivo assays of pharmaceutical libraries, leads to better understanding of tumor behavior, and helps to identify novel therapeutic targets.
Louise A. Mawn, MD, Vanderbilt University Medical Center, Nashville, Tennessee, USA, discussed ocular adnexal lymphoma and the impact of monoclonal antibodies on disease survival. Dr Mawn's key message stated that lymphoma is an insidious disease that can destroy bone, and, when treating isolated orbital lymphoma, consideration should be given to the patient's systemic health, comorbidities, and values.
Mucosa-associated lymphoid tissue (MALT) accounts for 80% of primary ocular adnexal lymphoma, and B-cell lymphoma accounts for 85% of all lymphomas. Therapeutic strategies are associated with unique short-and long-term efficacy and toxicities. Most treatment approaches fall into the area of chemotherapy, immunotherapy, radiation, or combinations of these agents. Local disease is often treated with orbital radiation only; more advanced disease may require immune-radiotherapy with chemotherapy. In many cases of MALT lymphoma, there is a previous medical history of inflammation or autoimmune disorders.
Diagnosis can be difficult. Lymphoma can have restricted diffusion but is not typically rim enhancing in immunocompetent patients. Treatment of B-cell lymphoma of the orbit should start with rituxan alone for 4 weekly doses; if ineffective, chemotherapy should be added. Radiation therapy should be reserved in cases in which neither of these approaches is effective. The use of rituxan has led to a 20% gain in remission rates. Other agents likely to improve response and survival are the oral B-cell receptor inhibitors.
Philip Custer, MD, Washington University, St. Louis, Missouri, USA, was invited to present the 2014 Wendell Hughes Lecture. He discussed “The Spectrum of Prostaglandin Orbitopathy.”
Latanoprost, bimatoprost, travoprost, tafluprost, and unoprostone are synthetic prostaglandin F2α analogs and are the preferred agents for initiation of glaucoma therapy [Wilson MR et al. Am J Ophthalmol. 2008]. These medications should not be used in patients with intraocular inflammation or cystoid macular edema; they also tend to increase iris pigmentation and the length and thickness of eyelashes.
Dr Custer noted that a variety of adverse events (AEs) have been noted since the introduction of these agents. These AEs include deepening of the lid sulcus [Peplinski LS and Albiani SK. Optom Vis Sci. 2004], periorbital fat atrophy, deepening of the upper eyelid sulcus, relative enophthalmos, and loss of lower-eyelid fullness. Involution of dermatochalasis was reported in 5 patients from chronic topical daily use of bimatoprost [Filippopoulous T et al. Ophthal Plast Reconstr Surg. 2008]. In addition to marginal eyelid thinning, Dr Custer is seeing more patients with cicatricial entropion, meibomian gland dysfunction, and lash ptosis. A more recent study has confirmed an association between prostaglandin analog use and a higher incidence of ptosis, levator muscle dysfunction, and low lid retraction [Shah M et al. PloS One. 2013]. Signs and symptoms of these conditions recede when treatment is stopped.
Prostaglandin-associated periorbitopathy (PAP) is the name given to the constellation of eyelid and orbital changes that accompany the administration of topical prostaglandin analog eye drops. There is concern among clinicians that PAP can interfere with examinations, applanation tonometry, and treatment. It has been hypothesized that tight orbit syndrome is a consequence of treatment with prostaglandin analogs. A poster presented at this year's conference showed that topical bimatoprost increases eyelid tension and causes narrowing of the eyelid sulci fissure [Kent TL Custer PL. AAO 2014. PO169]. Dr Custer remarked that the increased use of nonglaucoma topical medications such as antibiotics, steroids, and medications such as Restasis might be due to inflammation associated with prostaglandins. In a study that reported the safety of latanoprost use throughout 5 years, inflammation was a common AE, along with ocular irritation (34.5% of patients), hyperemia (28.9%), blepharitis (12.4%), and conjunctivitis (10.3%) [Alm A et al. Arch Ophthalmol. 2004].
An animal study showed that high levels of bimatoprost are absorbed in ocular tissues after short treatment periods [Woodward DF et al. J Pharmacol Exp Ther. 2003]. A more recent study also reported that prostaglandin analogs inhibit human preadipocyte differentiation and intracellular lipid accumulation, which may explain superior eyelid deepening when used in glaucoma patients [Choi HY et al. J Ocul Pharmacol Ther. 2012]. No studies have specifically addressed the incidence of these effects. In one study, however, PAP was seen in 93.3% of bimatoprost-treated patients, 70% of travoprost-treated patients, and 41.4% of patients treated with latanoprost [Kucukevcilioglu M et al. Clin Experiment Ophthalmol. 2014]. These findings support previous anecdotal evidence.
Dr Custer stated that prostaglandin analogs affect his practice on an almost daily basis by contributing to a variety of eyelid and orbital deformities. Because the effects are partially reversible, clinicians should consider discontinuation of these agents when possible. Future innovations such as new delivery methods and designer prostaglandin analogs are needed.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.