

Summary
The use of oxygen in the initial treatment of patients with suspected myocardial infarction (MI) dates back over a century. However, there is scant evidence for the benefit of oxygen in patients without hypoxia. The multicenter controlled AVOID trial compared routine supplemental oxygen with no supplemental oxygen on myocardial infarct size in normoxic (=?94%) patients with STEMI, as discussed in this article.
- cardiology clinical trials
- myocardial infarction
The findings from the Air Versus Oxygen in Myocardial Infarction [AVOID; Stub D et al. Am Heart J. 2012] study were presented by Dion Stub, MBBS, Baker IDI Heart & Diabetes Institute, Melbourne, Australia.
The use of oxygen in the initial treatment of patients with suspected myocardial infarction (MI) dates back over a century. However, there is scant evidence for the benefit of oxygen in patients without hypoxia [Cabello JB et al. Cochrane Database Syst Rev. 2010]. In fact, as little as 15 minutes of supplemental oxygen via a face mask may result in hyperoxemia, resulting in diminished coronary blood flow and increased coronary vascular resistance and reperfusion injury.
The multicenter controlled AVOID trial compared routine supplemental oxygen with no supplemental oxygen on myocardial infarct size in normoxic (≥ 94%) patients with STEMI. In the trial, 638 patients were assessed by paramedics for symptoms of STEMI and randomized 1:1 to receive oxygen at the rate of 8 L/min delivered through a face mask (n = 318) or no oxygen (n = 320). At hospital arrival, STEMI was confirmed in 218 patients receiving oxygen and 223 patients not receiving oxygen, and the randomized conditions were continued until the end of the primary percutaneous coronary intervention. In the no-oxygen arm, if saturation dropped < 94%, supplemental oxygen was added and titrated to a goal of 94%. As expected, the oxygen saturation level was consistently higher in oxygenated STEMI patients before hospital arrival and ≤ 4 hours after arrival. Cardiac enzymes were monitored for 72 hours, with cardiac magnetic resonance imaging (MRI) and clinical follow-up for ≥ 6 months.
The co-primary end point was myocardial infarct size based on mean peak levels of creatine kinase and troponin I and areas under the curve for these biomarkers. Clinical secondary end points included ST segment resolution, survival to hospital discharge, major adverse cardiac and cerebrovascular events (MACCEs; death, MI, revascularization, stroke at 6 months), and myocardial infarct size determined at 6 months by cardiac MRI.
Baseline characteristics, including the prevalence of cardiac arrest and cardiogenic shock, were comparable in the oxygen and no-oxygen arms. Procedural details were also similar between the groups (Table 1).
AVOID Study Procedural Details
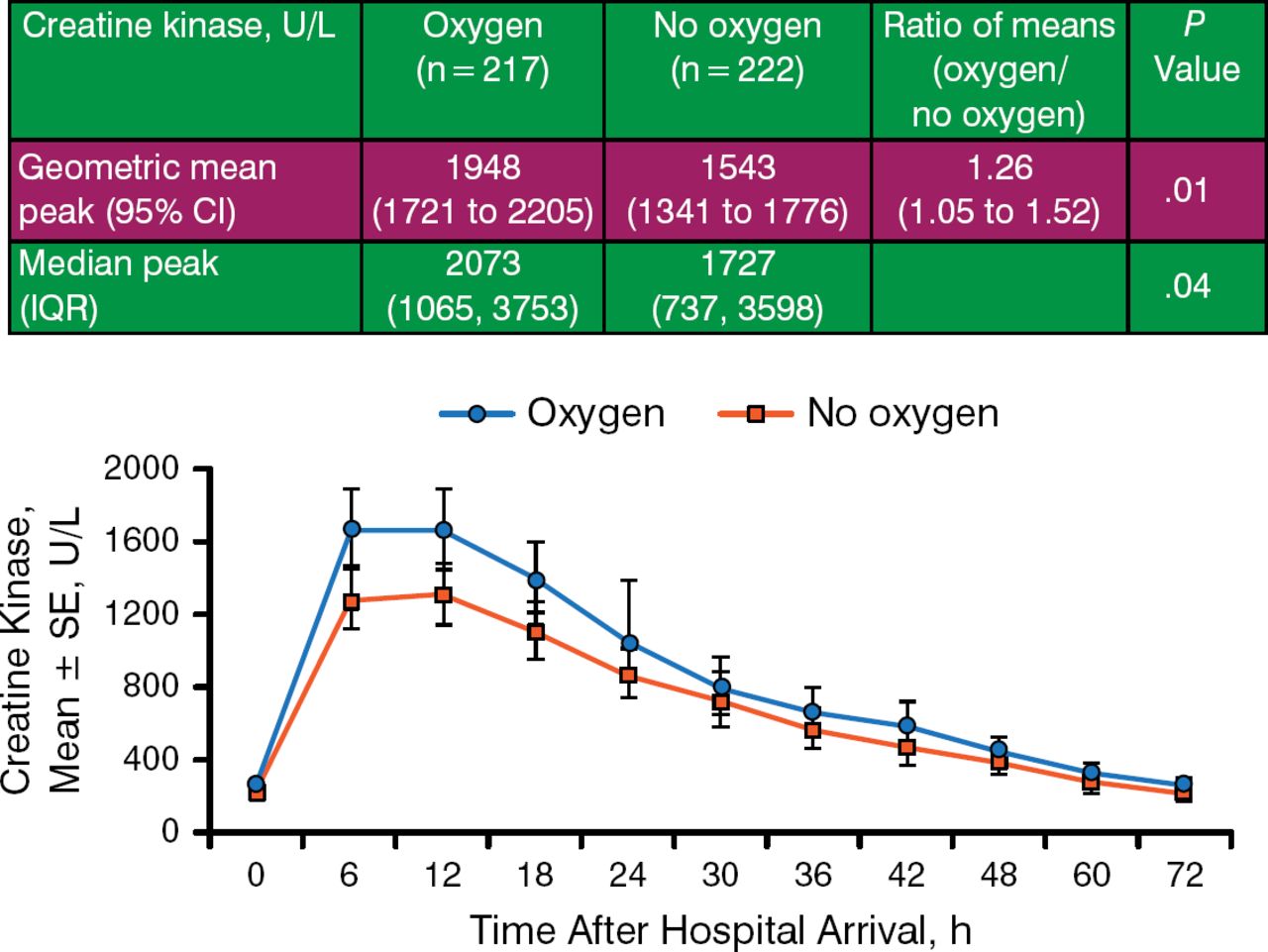
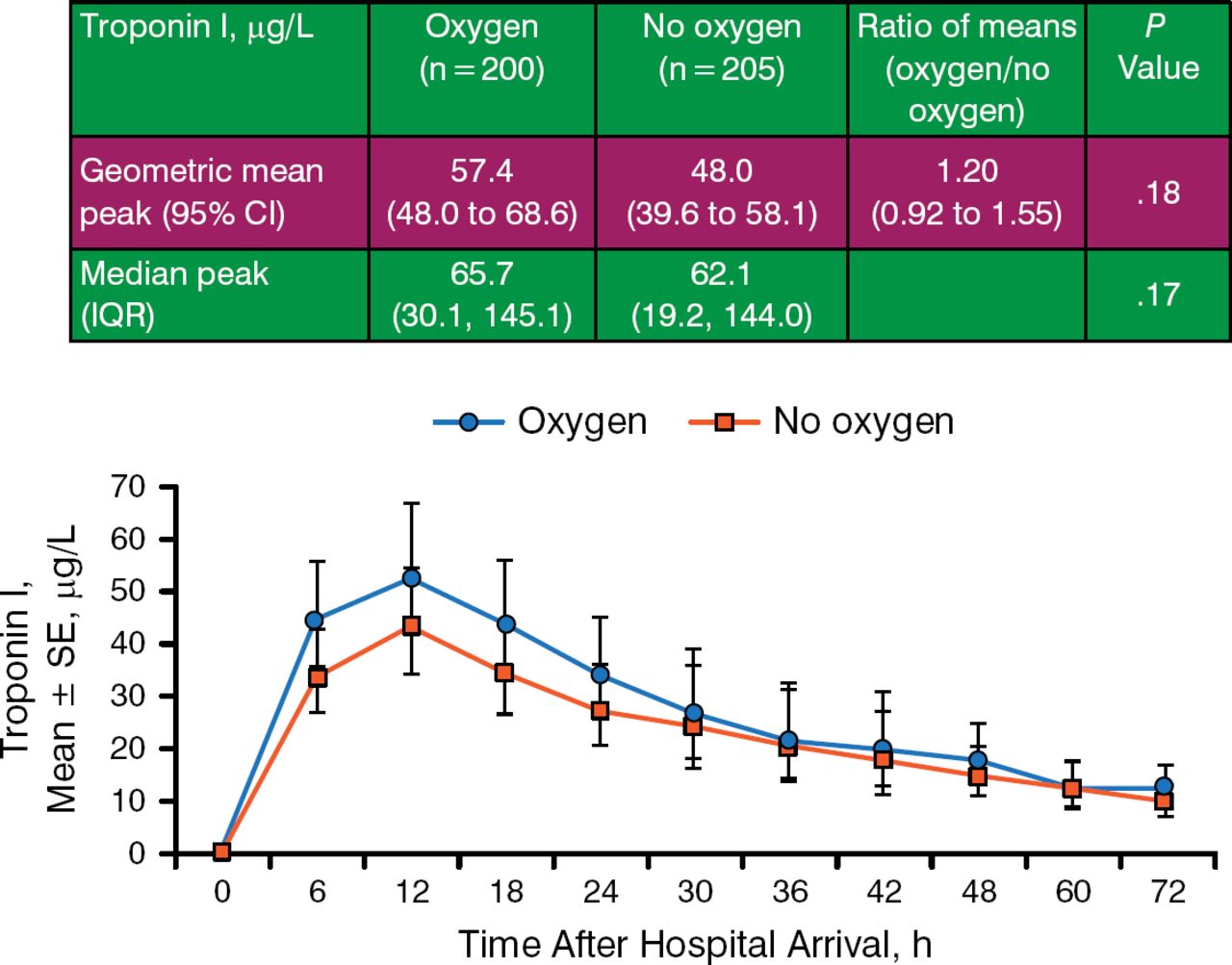
The use of oxygen was associated with a significant 26% increase in mean peak creating kinase, as well as an increase in area under the curve, suggestive of oxygen-related cardiac damage (Figure 1). The trend for troponin was similar, but the groups were not significantly different (Figure 2).

Creatine Kinase Values in the Study Groups
Area under the curve, P =.04.
IQR, interquartile range.
Reproduced with permission from D Stub, MBBS.

Troponin Values in the Study Groups
Area under the curve, P =.12.
IQR, interquartile range.
Reproduced with permission from D Stub, MBBS.
MRI was conducted at 6 months in 65 patients who had received oxygen and 74 patients who had received no oxygen. This revealed a trend toward increased cardiac infarct size as a proportion of left ventricle mass, indicative of scarring, between the oxygen and no-oxygen arms (12.6%; 6.7 to 19.2% vs 9.0%; 4.1 to 16.3%; P = .08).
The trial was underpowered to assess clinical end points; thus, all findings are considered exploratory. Supplemental oxygen use was associated with recurrent MI at hospital discharge (5.5% vs 0.9%). The trend continued to 6 months, although the result was less impressive (7.6% vs 3.6%). There was an association between MACCEs at 6 months in the oxygen arm (21.9% vs 15.4%). Mortality was low in both the oxygen and no-oxygen arms (3.8% vs 5.9% at 6 months).
The use of oxygen in STEMI patients was associated with greater myocardial injury, as assessed by creatine kinase (but not troponin), with a suggestion of increased recurrent MI and major cardiac arrhythmia and larger myocardial infarct size at 6 months. The findings question the current practice of supplying oxygen to all patients with MI.
- © 2014 MD Conference Express®
Tools









{kind=link}
{kind=link}
Table of contents
Cited By...
- No citing articles found.