

Summary
A systematic diagnostic and therapeutic algorithm, which includes urgent catheterization, following cardio-pulmonary resuscitation is feasible and is associated with improved patient outcome. This article presents results from a prospective study assessing a systematic approach to managing patients following resuscitation.
- Cardiology Clinical Trials
- Critical Care
- Myocardial Infarction
- Cardiology
- Cardiology Clinical Trials
- Critical Care
- Myocardial Infarction
A systematic diagnostic and therapeutic algorithm, which includes urgent catheterization, following cardiopulmonary resuscitation is feasible and is associated with improved patient outcome. Hubertus von Korn, MD, Krankenhaus Hetzelstift, Neustadt/Weinstrasse, Germany, presented results from a prospective study assessing a systematic approach to managing patients following resuscitation.
The survival rate after cardiac resuscitation is poor at approximately 8% [Nichol G et al. JAMA. 2008]. Current guidelines for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death from the American College of Cardiology/American Heart Association/European Society of Cardiology recommend consideration of immediate coronary angiography in patients with postcardiac arrest for whom an acute coronary syndrome (ACS) is suspected [Zipes DP et al. Circulation. 2006]. A systematic diagnostic and therapeutic approach, however, has not been tested.
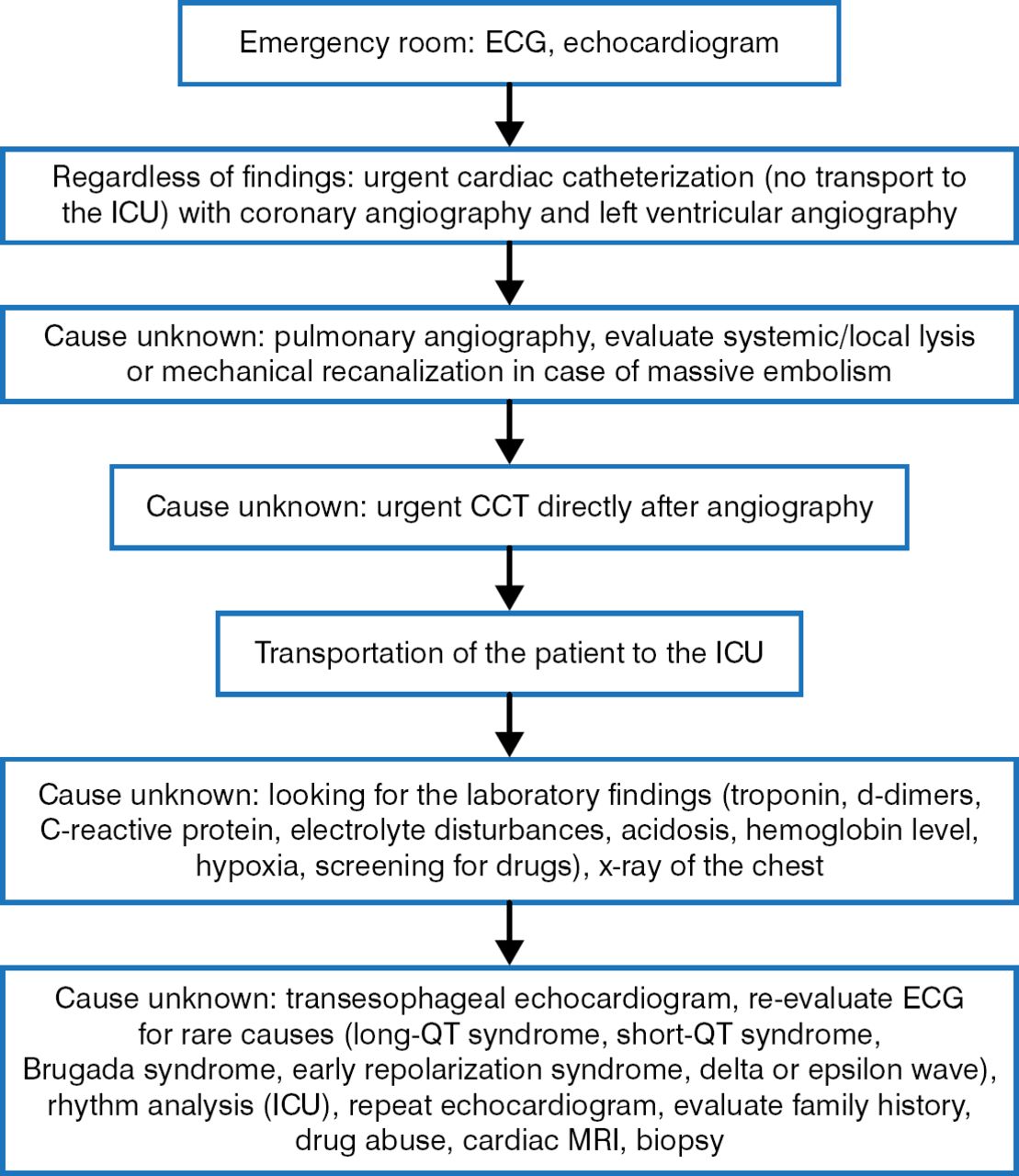
The systematic approach studied consists of an electrocardiogram and echocardiogram performed in the emergency room, urgent cardiac catheterization with coronary angiography and left ventricular (LV) angiography, pulmonary angiography if the cause of arrest is unknown, computed tomography of the chest and the head, predefined laboratory tests (if cause is unknown), establishment of an intra-arterial balloon pump (IABP), hypothermia, and cardiac magnetic resonance imaging (Figure 1).

Diagnostic Algorithm Used Following Cardiopulmonary Resuscitation
CCT, coronary computed tomography; ECG, electrocardiogram; ICU, intensive care unit; MRI, magnetic resonance imaging.
Reproduced with permission from H von Korn, MD.
Over 5 years, 212 patients were enrolled in the protocol for the prospective study. The primary end point of the study was the Cerebral Performance Category Scale. The mean patient age was 66.7 years, men comprised 71.2% of the study population, and the mean LV ejection fraction was 42.9%. The mean time from first alert to arrival of the mobile emergency medical unit was 7.7 minutes, the mean time from first alert to time to arrival in the clinic was 50.1 minutes, and the mean time from first alert to cardiac catheterization was 76.6 minutes. The first detected rhythm was ventricular fibrillation in 99 patients (46.7%); critical bradycardia, electromechanical dissociation, or asystole in 96 (45.3%); and ventricular tachycardia in 5 (2.4%). The rhythm was not classified in 12 patients (5.7%).
Ninety percent of patients had a cardiac cause of their event (47.2% with an ACS and 42.9% with other cardiac causes). Other cardiac causes included cardiomyopathy (20.8%), lung embolism (3.8%), Tako-Tsubo cardiomyopathy (3.3%), and others (15.1%), which included coronary artery disease without non-ST or ST elevation (7.1%), and long-QT syndrome or early repolarization (2.8%). The 2 main noncardiac causes were intracerebral bleeding and sepsis. A significant coronary artery stenosis, defined as a percentage of diameter stenosis > 60%, was found in 130 (61.3%) and a percutaneous coronary intervention (PCI) was performed in 101 (47.6%) of these patients.
In the intensive care unit, 20 patients (9.4%) had IABP, 55 (25.9%) underwent hypothermia, and 23 (10.9%) had an implantable cardioverter defibrillator or pacemaker implanted. The survival rate was 35.9%, and 67 patients (31.8%) had a cerebral performance category scale of 1 or 2, indicating good cerebral performance or moderate cerebral disability.
In patients treated with PCI, a significant decrease in mortality was found for patients with restoration of TIMI 2 or 3 blood flow compared with TIMI 0 or 1 flow (65.4% vs 95.7%; P < .01). Mortality for patients treated with hypothermia was 52.7% compared with 68.2% for no hypothermia (P = .04). There was a trend for neurologic benefit among patients treated with hypothermia: 40% in this group had a cerebral performance category scale of 1 or 2, compared with 28.9% not treated with hypothermia (P = .05). Establishment of an IABP had no effect on mortality (P = .6), which was 70.0% in those with and 63.6% in those without an IABP established.
- © 2014 MD Conference Express®
Tools









{kind=link}
Table of contents
Cited By...
- No citing articles found.